For the freedom to have control of one’s body – Promoting and ensuring access to women’s sexual and reproductive health and rights in sub-Saharan Africa


Twenty-six years after the World Conference on Women’s Rights in Beijing, the Generation Equality Forum marks a crucial new stage in governments’ commitment to gender equality. The fight for gender equality remains an open issue at the international level. In a quarter of a century, there have been no new international texts to back up the previous commitments. Worse, the defence of women’s rights is hampered in many international forums by motley coalitions of governments that deny, for various reasons, the discrimination suffered by women. In cultural, social and religious contexts, women are denied control over their own bodies.
At the same time, the understanding of the mechanisms of discrimination against women has increased. The freedom to have control of one’s own body is often narrowly understood as the choice to procreate. But it is really about a wider set of rights, that are independent of each other, without which there is no autonomous choice or real equality: access to education and information, access to health care systems, access to contraceptive methods, access to legal and safe abortion, protection against sexual violence, such as rape, female genital mutilation, of child marriage, forced marriage, etc.
These rights form a continuum now referred to as Sexual and Reproductive and Health Rights (SRHR). The promotion of these rights, which faces many obstacles in the multilateral international framework, is the subject of particular mobilization by a broad coalition of governments, of which France is a member. In Paris, France, which is co-chairing the Generation Equality Forum with Mexico, will be particularly involved in the coalition on « Bodily Autonomy and Sexual and Reproductive Health and Rights ». This commitment, consistent with the affirmation of feminist diplomacy over the past several years, has raised substantial expectations on the part of many civil society organizations and partner countries involved in gender equality. To be fully mobilizing, this French commitment must be translated into a specific financial effort within the framework of official development assistance. Budgetary choices, from this point of view, have fallen short of the message’s objectives.
A strengthening of the French commitment is all the more necessary as the health and security contexts are deteriorating in the regions where it counts. Women’s and girls’ rights are particularly vulnerable to the security, political, economic and cultural vagaries of societies experienced in sub-Saharan African countries on a daily basis. We have observed that, as a result of the Covid-19 pandemic, advances in sexual and reproductive health and rights are difficult to achieve and their decline is particularly severe when access to the school system is made impossible, when the health care system is disorganized, when local associations no longer have the resources to carry out their actions, or when such rights are even directly hindered by certain social forces or by political or religious leaders. The resulting gender inequalities perpetuate and reinforce violence against women and girls.
However, if women and adolescent girls are denied the right to take control of their bodies, the repercussions are not limited to the loss of bodily autonomy. It is their entire emancipation journey that is at stake, with multiple impacts that concern their entire lives. These barriers threaten their future and the possibility of aspiring to a full education and economic independence, and deprive them of rights as basic as the right to health and security. In short, they deprive them of a fundamental universal right, their freedom and their right to choose.
It is therefore essential that societies and policy makers are made aware of the importance of promoting access to SRHR for women and girls and that funding in this area continues and is increased. This is why France’s official development assistance for SRHR in sub-Saharan Africa is essential to bring about tangible and continuous change on the ground with a view to guaranteeing these rights.
This report gives a voice to actors in the field who are developing concrete programmes to promote SRHR in five sub-Saharan African countries (Burkina Faso, Mali, Niger, Democratic Republic of Congo, Senegal). Thanks to numerous interviews with political and institutional leaders, representatives of local NGOs based in the five countries studied and French feminist associations, the work group identified several levers for action that still need to be developed to enable women to assert their rights.
The report makes six recommendations to the French government regarding funding for sexual and reproductive health and rights in sub-Saharan Africa:
1. Increase French funding for SRHR
2. Cover the full range of SRHR issues to meet needs on the ground: a priority for respecting women’s and girls’ fundamental rights
3. Simplify the process of identifying and accounting for funding for SRHR
4. Favour the funding of projects with a long timeframe
5. Adapt funding eligibility procedures for local and feminist NGOs
6. Invest in the potential of youth.
For the freedom to have control of one’s bodyPromoting and ensuring accessto women’s sexual and reproductive healthand rights in sub-Saharan Africa
This report written by Deborah Rouach was produced by a working group consisting of Amandine Clavaud , Juliette Clavière and Alexandre Minet for the Jean-Jaurès Foundation , and Suzanne Gorge and Marc-Olivier Padis for Terra Nova .
Executive summary
LIST OF ACRONYMS
AFD : French Development Agency
AU : African Union
CNJFL : Nigerian Cell of Young Female Leaders
CSE : Comprehensive sexuality education
CSO : Civil society organisation
DAC : Development Assistance Committee
DRC : Democratic Republic of Congo
FFM : French Muskoka Fund
FGM : Female genital mutilation
FP : Family planning
GBV : Gender-based violence
GEF : Generation Equality Forum
GNI : Gross National Income
HDI : Human Development Index
HIV : Human immunodeficiency virus
NGO : Non-governmental organisation
ODA : Official development assistance
OECD : Organisation for Economic Co-operation and Development
RMNCH : Reproductive, maternal, new-born and child health
RMNCAH : Reproductive, maternal, new-born, child and adolescent health
SDG : Sustainable development goal
SRH : Sexual and reproductive health
SRHR : Sexual and reproductive health and rights
STI : Sexually transmitted infection
UN : United Nations
UNFPA : United Nations Population Fund
FOREWORD
2021 represents a pivotal year for the defence of women’s and girls’ rights, especially the right to have control over their bodies. Indeed, while the coronavirus crisis has exacerbated the fragility of health services around the world, attacks on the sexual and reproductive health and rights (SRHR) [1] of women and girls are increasing and threatening to undermine and violate these fundamental rights in many parts of the world.
The holding of the Generation Equality Forum (GEF) in Mexico City in March 2021 and in Paris in June 2021 puts the defence of gender equality at the heart of the international political agenda and is therefore a major event. Although it does not aim to adopt a normative text, the Generation Equality Forum provides a framework for discussion for governments, civil society, the private sector and all individuals and organizations involved in the defence of women’s rights. It also provides the framework for concrete commitments by the participants, including the French government, which has taken a « champion » position within the coalition on the subject of SRHR.
To get around the blockages of multilateral negotiations, the Generation Equality Forum proposes an alternative method through « action coalitions » which bring together on an equal footing a multitude of private and public actors from all over the world whose representations and political actions converge. The issue of sexual and reproductive health and rights (SRHR) will be specifically addressed in one of these action coalitions, a significant stance given that since the 1995 World Conference on Women in Beijing, “no international conference or discussion on this [topic] has been deemed possible by governments and civil society, for fear of a negative effect on these rights” [2] . Indeed, in the absence of a political perspective and international consensus on SRHR, addressing this issue within the framework of the Generation Equality Forum can reinforce initiatives involving a wide range of actors.
The format of the Generation Equality Forum marks a number of departures from traditional international diplomacy. This is not a multi-stakeholder framework that is binding on all stakeholders, but a voluntary participation that allows for collaboration between partners. In this way, it promotes innovation, concrete steps and financial commitments to achieve this and ensure a wider outreach beyond governmental bodies. France, given its historic role as an advocate for women’s right to have control over their own bodies and as a donor of official development assistance to Africa, should be encouraged to make concrete, sustainable commitments to sexual and reproductive health and rights at the Generation Equality Forum.
Introduction
On 8 March 2021, on the occasion of International Women’s Rights Day, Phumzile-Mlambo-Ngcuka, Executive Director of UN Women declared: "While progress has been made over the past twenty-five years, no country has achieved gender equality” [3] . Moreover, according to initial assessments of the current health crisis, the latter is resulting in a significant decline in SRHR: “47 million women could lose access to contraception, resulting in 7 million unwanted pregnancies [4] ”.
Yet gender equality and women’s sexual and reproductive health (SRH) are recognized as fundamental rights by international bodies. The Convention on the Elimination of All Forms of Discrimination against Women in 1979, the International Conference on Population and Development in 1994, the Beijing Declaration and Platform for Action in 1995, a world conference on women’s rights, whose twenty-sixth anniversary the Generation Equality Forum (GEF) will celebrate, and the 2015 Sustainable Development Goals (SDGs) formulated as part of the 2030 Agenda, are founding texts in this field. However, the subject of SRHR is a source of much tension both within governments and at the international level. In multilateral bodies, some governments are challenging the recognition of these rights and the implementation of programmes to support them. Even within civil society, religious representatives defend representations of the family and the procreative role of women that go against freedom of choice. This is why there is a power struggle between governments and within intergovernmental organizations over the protection rights of women’s right to bodily autonomy. In the absence of consensus, it is proving extremely difficult to obtain the adoption of binding commitments in favour of SRHR.
There are significant disparities in access to SRHR across the world. France is strongly committed to raising the profile of this issue at the international level and to promoting comprehensive, long-term progress in SRHR in developing countries where France is involved and where the needs are highest, notably in sub-Saharan Africa. The integration of the SRHR concept into the French government’s official language dates back to the 2010s. For a long time, development aid policies focused on protecting mother and child health, but the official discourse then shifted to a demographic dividend approach [5] for sub-Saharan Africa. This discourse, which often led to a demographic “risk” being highlighted, could be seen as a form of interference from another era by France’s partners. More recently, France has prioritized SRHR in the framework document L’Action extérieure de la France sur les enjeux de population, de droits sexuels et reproductifs 2016–2020 [6] , demonstrating a change in perspective, in line with recommendations from civil society organizations (CSOs). This new approach is part of the promotion of a feminist diplomacy upheld by France. As part of its co-chairing of the Generation Equality Forum with Mexico and its leadership of the “Bodily Autonomy and Sexual and Reproductive Health and Rights” coalition, concrete commitments are expected from France to initiate tangible changes in terms of gender equality and access to SRHR for the next five years.
This report therefore analyses the implications of this new diplomatic approach, in particular French financial commitment to SRHR in five sub-Saharan African countries: Mali, Senegal, Burkina Faso, Niger and the Democratic Republic of Congo [7] . In these countries, the rights of girls and women to bodily autonomy are fragile, threatened and even violated. These are inalienable rights of women that are essential for their empowerment. SRHR are a crucial element in achieving gender equality and ensuring an equitable future for a population as a whole. In an often-dramatic context for girls and women in this region, this report reiterates the need to actively promote and defend free access to SRHR and comprehensive sexuality education (CSE) for women and the general population. We also study the multiple economic, cultural, religious, security and health crisis-related obstacles against which a broad mobilization of governments and civil societies is, more than ever, necessary. Finally, we give actors mobilized in the field an opportunity to express themselves, who emphasize the importance of the approach in terms of access to rights to support aspirations and change in these countries. The report concludes with six recommendations to the French government regarding its official development assistance for SRHR in sub-Saharan Africa.
1. ADDRESSING SEXUAL AND REPRODUCTIVE HEALTH AND RIGHTS PRIORITIES IN SUB-SAHARAN AFRICA [8]
A. DEFINITION OF SEXUAL AND REPRODUCTIVE HEALTH AND RIGHTS
First of all, it should be noted that the very notion of SRHR represents progress in that it considers these rights as a whole, taking a holistic approach [9] . SRHR bring together a set of different but complementary concepts. It is the notion of linking a health approach with a freedom approach through access to a certain number of rights. SRHR therefore include sexual health, reproductive health, sexual rights, and reproductive rights. The issues to which these concepts refer are multiple and can be broken down as follows:
– family planning
– having control over one’s own body
– the right to choose whether or not to have sexual relations, when and whom to marry, whether or not to have a child, how many children to have and when to have them
– access to sexual and reproductive health care
– the right to safe and legal abortion
– respect for the integrity of the body, i.e. the fight against female genital mutilation and all other forms of gender-based sexual violence
– access to comprehensive sexuality education (CSE) and information on SRHR
– information about all SRHR issues
– the right to a safe sex life, i.e. combating sexually transmitted infections and diseases (STIs)

Source for table: Recommendations for the ICPD beyond 2014: Sexual and Reproductive Health and Rights for All, High-level Task Force for the International Conference on Population
and Development (ICPD), High-Level Task Force for ICPD, 2013, p.4.
Because of the intertwining of these themes, the term « care continuum » is used. This expression makes it possible to promote an integrated, cross-cutting approach to SRHR perceived as a whole without hierarchy and without exclusion. This approach emphasises a continuum of care and of information provided about SRHR, starting in childhood, through the school system, and aimed at the whole population without discrimination on the basis of gender, age, religion or social class. It puts forward a conception of SRHR in which the well-being of women and girls is seen as a whole, that includes physical, mental, emotional and social well-being. The decompartmentalization of SRH care services is another feature of this approach and responds to the realities of bodily autonomy where needs cannot be segmented as they are so plural and often linked to each other.
As a result, commitment to SRHR does not translate into a single type of programme or support action, but rather a multiplicity of programmes addressing each aspect. SRHR therefore imply both a diversity of commitments and a coherence to be sought across all these programmes. Access to education and health systems is the basis of this approach, but it is implemented through projects of varying scales and sometimes very targeted, small-scale field actions that nevertheless have a decisive impact on the target populations.
B. PRESENTATION OF THE REGIONAL CONTEXT IN TERMS OF SRHR
Sub-Saharan Africa is one of the regions in the world where access to SRH services and women’s right to control their own bodies is most precarious. The patriarchal organization of societies shapes mentalities and participation in social life and the full exercise of rights are limited by multiple forms of gender inequality and discrimination against women and girls.
In addition, the region suffers from a severe lack of resources to meet a high demand. This reinforces the infringements on the integrity of these rights. These can take the form of child marriage or forced marriage for adult women, pregnancy in a minor and/or unwanted pregnancy, female genital mutilation (FGM), gender-based sexual violence (GBV), and also an insufficiency or absence of SRH care (prevention, information, the fight against STIs, comprehensive sexuality education, lack of care, follow-up and management during pregnancy, childbirth and the neonatal and postnatal period, etc.). These denials of rights for adolescent girls and women are barriers to their independence and affect their entire lives.
In Central and West Africa, populations are facing multiple crises. Among them, the security situation in some of the countries studied constitutes a considerable obstacle to compliance with SRHR. Women and girls in conflict zones are exposed to war-related violence and in particular to sexual violence (rape, genital mutilation, prostitution, etc.). Insecurity therefore has major repercussions on access to care and information on SRHR and consequently on respect for women’s bodily autonomy. Mali, Senegal, Burkina Faso, Niger and the Democratic Republic of Congo (DRC), are all theatres, at different levels, of violence with terrible consequences for their populations. The resources devoted to stabilizing areas of conflict and fighting terrorism mean that basic public services, such as those relating to health, are lacking or non-existent and that people are deprived. SRH services are directly affected by insecurity and political instability, which hinder the establishment of effective, long-term health programmes. Moreover, regions that are difficult to access or dangerous are abandoned both by members of associations and NGOs worried about the attacks [11] that they could suffer because of their actions relating to SRHR, and by donors who fear a lack of transparency in the use of funding.
In West Africa, between 2007 and 2018, only 38% of adolescent girls and women aged 15 to 49 were able to make their own decisions about health, contraception and sex with their partners or spouses, three criteria which characterize bodily autonomy [12] . However, this figure drops drastically when looking at the countries in our study with 7% for Senegal and Niger, 8% for Mali and 20% for Burkina Faso [13] . The DRC is closer to the average for Central Africa (33%) with 31% of women and girls aged 15 to 49 declaring that they had bodily autonomy [14] . For the period 2015–2019, more than 6.5 million unwanted pregnancies were recorded in West Africa [15] . In addition, according to Guttmacher data [16] , between 2015 and 2019, 8 million abortions were performed in sub-Saharan Africa, three quarters of which were unsafe, possibly resulting in medical complications or even death. In Burkina Faso, 72% of abortions were performed by non-medical staff, as were 63% of abortions in Senegal.
The legislative framework for SRHR in West and Central Africa
The establishment of a legal framework would appear to be a prerequisite for ensuring an environment where women and girls’ rights are protected. Regional treaties have been adopted to ensure a favourable legal framework for the respect of SRHR in the region. For example, the Maputo Protocol signed in 2003 by the African Union (AU) to promote equal rights for girls and women recognizes abortion as a fundamental right in cases where the pregnancy is the result of rape, incest, endangers the woman’s mental and physical health or her life, and if the foetus has dangerous abnormalities.
In 2011, the Ouagadougou Partnership [17] was created between the nine French-speaking West African countries of Benin, Burkina Faso, Côte d’Ivoire, Guinea, Mali, Mauritania, Niger, Senegal and Togo, and donors, including the French Development Agency (AFD), to establish and strengthen family planning (FP). The aim is to enable wider use of contraception and to coordinate projects between countries and their funding partners. These treaties are especially important as they consolidate uniform legislation to protect the rights of women and girls across the region.
However, governments’ commitments under these regional treaties are not always transposed into national law. This is particularly the case for the DRC, which had signed the Maputo Protocol without publishing it in its Official Gazette , thereby impeding its application by the countries’ courts. It was not until 2018 that this transcription of the Maputo Protocol was adopted and that it took precedence over national law. However, it remains relatively unknown by the population. In Senegal, the protocol has been transposed into the country’s law, but local associations note that it is not respected [18] .
The legal framework is thus still far from homogeneous across the region, as illustrated by the case of abortion legislation (see box on following page). Even when the law allows abortion under certain conditions, its application continues to be a struggle and access to a medical center or competent personnel remains difficult. Access to contraception and the whole SRHR package also depend on the policy in each country.
Legal continuum | Southern Africa | Central Africa | East Africa | West Africa |
(N=5) | (N=9) | (N=18) | (N=16) | |
HIGHLY RESTRICTIVE LAWS | ||||
Category 1 | Angola | Mauritania | ||
Madagascar | Senegal | |||
None | Republic of Congo | |||
Sierra Leone | ||||
Malawi | Côte d’Ivoire ® | |||
Category 2 | Uganda | |||
Gambia (F) | ||||
To save a woman’s | Gabon (R, I, F)* | Somalia | ||
Mali (R, I) | ||||
life | South Sudan | |||
Nigeria | ||||
Tanzania | ||||
MODERATELY RESTRICTIVE LAWS | ||||
Category 3 | Burundi | Chad (R, I, F)* | ||
Comoros | ||||
To save a woman’s | Cameroon ® | Burkina Faso (R, I, F) | ||
Djibouti | ||||
life and preserve | Lesotho (R, I, F) | Equatorial Guinea +, ++ | Guinea (R, I, F)* | |
her health (without explicit mention | Ethiopia (R,I, F)** | |||
Central African Republic (R,I, F)* | Niger (F) | |||
of mental | Kenya | Togo (R, I, F) | ||
health) | ||||
Zimbabwe (R, I, F) | ||||
Category 4 | Eritrea (R, I)* | |||
To save a woman’s | Botswana (R, I, F) | DRC (R, I, F) | Mauritius (R, I, F) ++ | Ghana (R, I, F) |
life and preserve | Eswatini (R, I, F) | Mozambique (R, I, F)* | ||
her health (with explicit mention | Chad (R, I, F) | Liberia (R, I, F) | ||
Namibia (R, I, F) | Rwanda (R, I, F)* | |||
of mental | ||||
health) | Seychelles (R, I, F) | |||
BROADLY LIBERAL LAWS | ||||
Category 5 | ||||
To save a woman’s | ||||
life and preserve her | Zambia (F) | |||
(physical and/or | ||||
mental) health and for | ||||
socio-economic reasons | ||||
Category 6 | ||||
No restriction as to | Cape Verde § | |||
reason (with legal | South Africa § | Sao Tome and Principe § | ||
limits on gestational | Guinea-Bissau | |||
period and other | ||||
legal requirements) | ||||
Distribution of sub-Saharan African countries by sub-region and laws governing abortion
Most common additional reasons:
R = rape, I = incest; F = severe foetal impairment
Underage girls are eligible | + Marital consent required | ++ Parental consent/notification required | § Gestational limit of 12 weeks for abortions on request | ** No gestational limit specified for abortions on request.
NB: Many laws defining the legal basis for abortion are independent of a country’s categorization on the legal continuum. The most common are those that allow abortion in cases of rape, incest, or severe foetal impairment; these are listed here for the four categories for which these additional reasons logically apply. DRC = Democratic Republic of Congo. Sources: References 20–23.
Source: Akinrinola Bankole et al, From unsafe to safe abortion in sub-Saharan Africa: slow but steady progress, Guttmacher Institute, 2020
In Mali, for example, the law requires the signature of three doctors before an abortion can be performed, making access difficult, which is already restrictive within the legal timeframe, especially since doctors invoke the conscience clause. In Burkina Faso, it is necessary to wait for a court ruling that rape or incest has resulted in a pregnancy, with the result that the time period for a legal abortion cannot be respected [19] .
The heterogeneity of the legislative frameworks in the countries studied also works against women’s rights. This can be seen, for example, in the fight against gender-based violence. Mali is the only country in the region that does not prohibit gender-based violence, thereby allowing practices such as female genital mutilation to continue unimpeded. It suffices to take a woman from Senegal, Niger or Burkino Faso over the border to enable female genital mutilation take place. According to the United Nations Population Fund (UNFPA) report, 86% of Malian women aged 15 to 19 were mutilated between 2004 and 2018. Forty-five per cent of women aged 15 to 49 have experienced physical and/or sexual violence, according to the National Institute of Statistics in Mali [20] .
Another challenge is access to information about the legislation, as populations have little information or knowledge about SRH laws and therefore their rights in this area. In Senegal, the law on reproductive health dates from 2005 and allows, women to decide freely and with discernment the number of their children and the spacing of their births. It also implies the right to have the necessary information, the right to better health for all and the right to the services provided for this purpose” [21] . However, local associations consider that it is not being implemented [22] . In Mali, there is a law on SRH adopted in 2002 guaranteeing access to family planning and prohibiting the refusal to prescribe or force the use of contraception on a person of any age. This law also remains little-known by the population [23] .
Moreover, where legislative frameworks exist in favour of SRHR in the countries studied, they are nevertheless hampered by the weight of traditions, which are sometimes reinforced by a regional security context that continues to deteriorate. Gender-based violence against women and girls can also take the form of forced marriages and underage marriages, which constitute a major obstacle to women’s empowerment. According to the UNFPA report, 39% of girls are married before they reach the age of majority in Central and West Africa [24] .

Source : Unicef, La situation des enfants dans le monde, 2016. Infographie : Le Figaro.
These practices particularly affect the most vulnerable, such as internally displaced persons and those living in conflict zones. Marriages of minors are most often carried out for economic reasons by families unable to provide for their children and lead to many early pregnancies and forced marriages. In 2020, 5.5 million people were internally displaced in the DRC, the largest number in the world [26] . These people living in camps constitute a segment of the population at risk due to the loss of their usual environment, the break in family and social ties linked to displacement and the increased weight of the community within the camp. This is why they are targeted and integrated into the actions by NGOs that implement awareness-raising sessions on SRH. Governments are also working with external partners to implement national plans to address the specific needs of these populations and develop integrated SRH services.
In Niger, the law allows girls to marry at the age of fifteen, compared to eighteen for boys, but they are often married at twelve [27] . The main explanation lies in the customs and honour dimension of marriage for families who want to avoid an out-of-wedlock pregnancy at all costs [28] . It should also be taken into account that having a large number of children in a household is perceived as being good for a family’s reputation. Moreover, in a context of great poverty, marriage is seen as a path to economic prosperity and improved social status within the community. Finally, despite progress in schooling, marriage still often appears to many families as the only possible choice for girls [29] .
The weight of customs and religion
There are many barriers to the development of SRHR in this region. Sometimes linked to political contingencies and the agendas of political leaders, they are also the consequence of a very strong prevalence of religious rules and a patriarchal vision of society.
Indeed, some governments and politicians have not made gender equality a priority in public policies, and in particular SRHR which touch on subjects that are still taboo in societies and which crystallize debates. When an area of SRHR is taken into account by the authorities, they prefer to use semantics that diminish the scope of the subject matter, for example, comprehensive sexuality education (CSE) is referred to as “family life education” in Burkina Faso.
Governments or political figures who favour SRHR may be criticized or even threatened by segments of society and influential conservative groups such as some religious and community leaders. In Senegal, for example, religious lobbies are active in the government and block progressive discourse on legalizing abortion in cases of rape and incest and on sexual and reproductive health in general.
In Mali, where the population is 90% Muslim, several initiatives related to SRHR have been cancelled. An attempt to include SRH issues in school textbooks was denounced by some religious leaders to President Ibrahim Boubacar Keïta; they argued that the “acceptance of differences” in the textbooks would encourage homosexuality [30] . The Malian government was obliged to abandon the project. In 2021, the draft law against gender-based violence proposed by Bintou Founé Samaké, the Minister for the Promotion of Women, Children and the Family, suffered the same fate.
According to the NGO, the Pananetugri Women’s Well-Being Initiative, in Burkina Faso, “in 2018 the Minister of Health, Nicolas Meda, raised the idea of granting the right to safe abortion with the President of the National Assembly. Once this was publicly reported in the press, there were strong reactions forcing the government to retract the suggestion". [31] Thus, in the face of traditions and pressure from a section of society and some religious leaders, attempts at legislation are thwarted and SRHR are passed over in silence. It is crucial to convince elected politicians that investing in health and SRHR is a right and a need, but above all a long-term investment that must be defended against prevailing traditions and customs. [32]
The influence of traditional and religious leaders and traditional rules on society can be seen in the daily lives of citizens, in the public space and in power relationships. In Burkina Faso, the chefferie (chieftainship) is omnipresent in the rural territories of the Centre and East, is no less absent from the major urban centres. However, their influence expresses less a replacement of the public authorities than a superposition of moral, sacred, and sometimes political authorities. For foreign and local NGOs, and for international representatives, any visit and/or implementation of projects must be preceded by a preliminary exchange with traditional and religious authorities, in order to introduce themselves and to foster acceptance and ownership of the project. This protocol ceremony is carried out in addition to the one that nevertheless retains primacy, with the local political authorities (governor, president of regional councils, mayor, etc.).
“Every time we go on a mission outside the capital of Burkina Faso, we first visit the administrative, political, traditional and religious authorities to present the reason for our presence and our mission. The religious authorities have a major influence on society” [33] . Moreover, “representatives of traditional and religious authorities are members of the Global Fund’s Country Coordinating Mechanism (CCM) for grants to defeat HIV, TB and malaria, along with France and other partners” [34] .
Community and religious leaders, who are almost always men, have a significant influence on people’s personal lives and how everyday matters are conducted. Women and girls are therefore particularly vulnerable in geographical areas where religious and cultural values weigh heavily on people’s lives. Many religious and conservative communities define acceptable and unacceptable behaviour. They perpetuate unequal and discriminatory gender roles for women and girls who must be subservient to the head of the family and fulfil their function as wives and mothers 1 . Marrying and having children, in this case, is not a woman’s choice, but a duty. In addition, communities impose practices that are harmful to the bodies of women and girls, such as female genital mutilation (FGM), of which female circumcision is the most common form, that violate their physical integrity and have their origins in cultural, religious and social customs 2 . In West Africa, FGM is widely practised, although its prevalence varies between countries (see illustration below).
FEMALE GENITAL MUTILATION/CUTTING (FGM/C)

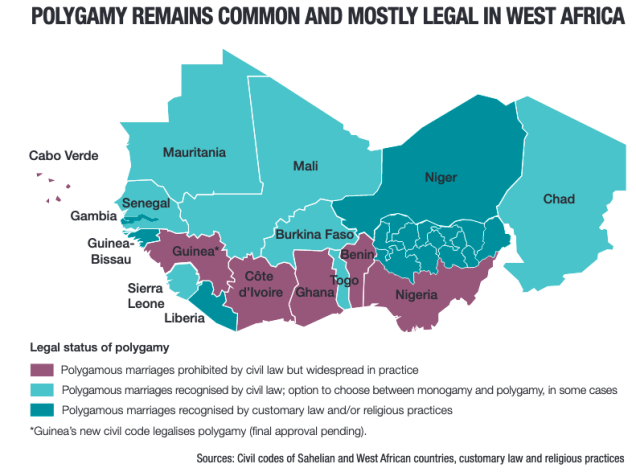
Furthermore, where customary law, religious practices and civic law are in agreement, the rights of women and girls are neglected and violated. This is particularly the case in all the countries in our study that legally allow polygamy, except for Niger. West Africa is the region where polygamy is most prevalent among the population: in Burkina Faso it is 36%, in Mali 34%, in Niger 29% and in Senegal 23% for the period 2010– 2018 [35] . In the DRC, polygamy is not widely practised, concerning only 2% of the population. The most common version of this practice is polygeny, where a man marries more than one wife, thus contributing to inequality between women and men.
In this context of widespread inequality and discrimination against women, including misogyny, male-controlled sexuality and social pressure on fertility, it is difficult for women and girls to access SRH care and information, to speak freely and confidently about their sexual and reproductive rights, and to claim these rights. SRH is also often considered to be a Western principle that is contrary to local values. The strength of these prejudices weighs particularly heavily on women and girls. However, gradual changes are taking place within more recent generations who are more able to demand their rights and have tools such as social media to inform themselves [36] .
Health systems in West and Central Africa
Numerous observations regarding the health system in these countries were made. The primary barriers between women and adolescent girls and SRH services are financial and geographical, especially for those living in rural areas, which range from 50% to over 70% depending on the country [37] . The presence of SRH services is uneven, with the peripheries being less equipped than the urban centres. Extending the national SRH programmes throughout the region is a real challenge, especially given the lack of resources and the instability of certain areas. The priorities are to strengthen health systems where they exist and ensure that good quality services are delivered.
The region’s health systems rely mainly on donations. Although countries committed in 2001 in the African Union’s Abuja Declaration to devote 15% of their national budgets to financing the health sector, 20% of which is dedicated to SRHR, this is still not the case for Niger, Burkina Faso, Mali, Senegal and the DRC [38] . National resources allocated to health are insufficient to meet the demand, so people have to pay for care. The population’s expenditure on health is therefore low because of the significant cost that medical care represents [39] . In 2018, the Human Development Index (HDI) for the countries in our study was extremely low: Mali’s HDI was 0.422/1, Niger’s was 0.341/1, Senegal’s was 0.494/1, Burkina Faso’s is 0.434/1, and the DRC’s was 0.459/1. In Burkina Faso, a strong commitment was made by the government in September 2020 to provide free medical consultations, family planning services and contraceptives.
However, people are still confronted with discretionary decisions by health workers, especially in rural areas. In health centres, women and girls may be subject to the prejudices and moral representations of medical staff on SRH issues, which can interfere with diagnoses and care. Some refuse to prescribe or give access to a contraceptive method if the person is not married, considering that sexual relations outside of marriage are prohibited, whereas the law does not state anything of the sort. As Fatou Ndiaye Turpin, Executive Director of the Réseau Siggil Jigéen, reminds us, "the 2005 law on reproductive health recognizes that the right to reproductive health ‘is a fundamental and universal right guaranteed to every human being without discrimination on the basis of age, sex, wealth, religion, race, ethnicity, marital status or any other situation.’ There are no legal restrictions on young people’s access to contraception and other basic health services, such as pregnancy and STI testing, except for the requirement that they must be at least 15 years old to consent to HIV testing” [40] . The contraceptive prevalence rate remains a real challenge in a context in which sexuality outside marriage is still considered morally lax. The contraceptive needs of women aged fifteen to forty-nine are 58% satisfied in Burkina Faso, 56% in Senegal, 49% in Niger, 45% in Mali and 28% in DRC for the year 2021 [41] .
In other cases, medical care does not take into account women’s mental and physical suffering. As a result, there is a widespread lack of trust in health care workers [42] . This is particularly the case in Mali, where in hospitals « there is no pain treatment for women during childbirth: they lie on tables in a gynaecological position, in communal birthing rooms, with no consideration for their privacy or their physical and mental well-being; they cannot be accompanied in hospitals, so they give birth alone and sometimes they see each other die » [43] .
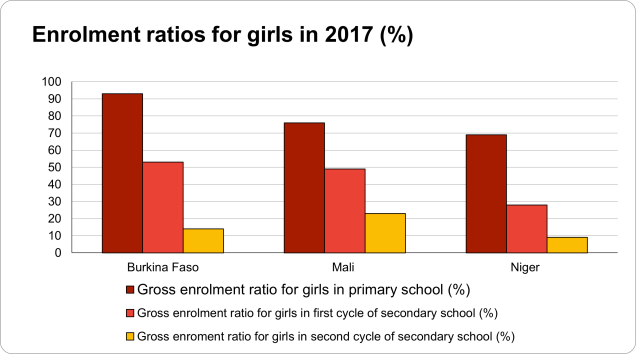
Girls’ education and schooling is a key element in the empowerment of girls and women. This gives them the ability to assert themselves, gain autonomy and make decisions about their bodies. Keeping girls in school helps prevent under-age pregnancies and gives them a future in which they gain skills to enter the labour market and contribute to the socio-economic development of the country [44] .
School is also the best place for young people to get information and advice on sexuality. Providing comprehensive sexuality education (CSE) in schools is therefore crucial to raising awareness among young people. However, across the countries surveyed in our report, sexual and reproductive health education is widely perceived as encouraging young people to have sex. Because sexuality remains taboo and subject to prejudices within families and society, the subject is passed over in silence, contributing to the exposure of young people to many dangers, misinformation and the persistence of false beliefs. As a result, the contraceptive needs of 47% of unmarried Senegalese women aged fifteen to forty-nine year-old were not satisfied in 2017 [45] . In 2018, in Mali, this was the case for 52% of single women and girls [46] .
Parents know that their children have sex in their teens, and so to avoid the possibility of pregnancy out of wedlock, they encourage or even force their daughters to marry early and therefore leave school. The schooling of girls and information on SRH appear to be essential to ensure their emancipation and their ability to make choices informed by the knowledge of their rights. The marriage of girls goes results in them leaving school, which has immediate and long-term consequences for their physical and mental well-being and economic empowerment: they are separated from their families, exposed to sexual violence and dependent on their husbands. The table below shows the significant decline in girls’ attendance between junior high and high school, at which age they are often withdrawn from school to be married. This is confirmed by the low female literacy rate in the countries studied in this report: in 2018, more than 50% of women aged 15 and over were illiterate in region [47] .
Source: UNESCO database.
The impact of Covid-19 on SRHR in West and Central Africa
The economic consequences of the pandemic will be particularly felt in the region. According to the World Bank, sub-Saharan Africa will be the second most affected region after South Asia, with an estimated 34 million additional poor people in the region [48] . The conditions created by the Covid-19 health crisis have exacerbated the already alarming situation with regard to sexual and reproductive health (SRH) services, which have been deemed « non-essential ». They have thus been rendered invisible, with financial resources being mainly dedicated to governments’ priority concerns. The closure of SRH services, including those for mother and child health, has been due to cases of contamination in health care centres, a shortage of family planning resources particularly in rural areas, insufficient staff since they were reallocated to Covid-19 treatment units or abandoned their posts for fear of being contaminated, as well as loss of funding, which has been allocated to services dedicated to fighting Covid –19 [49] . On the population side, there was also a drop in attendance at the centres due to travel restrictions, fear of contracting the virus, lack of confidence in the health care system and reduced income due to the health crisis. Both the supply of and demand for SRH services have therefore been affected by the health crisis.
Furthermore, women and girls have been the first to suffer the consequences of the pandemic as social control over their bodies has been reinforced. The study carried out by Equipop on the consequences of Covid-19 on women’s rights and health in West Africa reveals that there is « a return of a certain moralistic and conservative attitude towards young people’s sexuality, characterized by promoting abstinence and making women feel guilty » [50] . This discourages women and girls, especially the younger ones, from going to health centres to receive health services or to seek information. In addition, women and girls who have been obtaining contraceptives in secret are at risk of facing the disapproval of their spouses or families if this becomes known. The breakdown of services and information on SRHR intensifies the vulnerable situation in which young people and women find themselves. In addition, with the closure of schools, curfews and lockdowns resulting in the confinement of women and men in their homes, gender-based violence, such as rape, female genital mutilation, forced marriages and child marriages, has seen an unprecedented increase. The testimonies gathered from local NGOs are unanimous on this subject: women and girls are suffering the full force of the negative consequences of the pandemic, which affect their freedom to control their own bodies.
According to the UN, « 47 million women could lose access to contraception, resulting in 7 million unwanted pregnancies » [51] . Furthermore, according to the UN’s April 2020 predictions, « an additional 31 million cases of gender-based violence can be expected to occur if lockdown continues for another six months” [52] . This is in addition to »13 million additional child marriages between 2020 and 2030 2030" and « 2 million cases of preventable female genital mutilation » over the next decade. The UN Women report published in September 2020 concluded that « decades of progress towards gender equality could be lost in one year of the pandemic » [53] .

Source: PAI, Mitigating the impacts of Covid-19 in low and middle income countries, 2020.
The pandemic has thus seriously undermined progress made in recent years in the field of SRHR. Civil society actors have responded by developing innovative strategies to continue their efforts.
C. ACTIONS BY LOCAL CIVIL SOCIETY ORGANIZATIONS, COMMUNITIES AND POLITICAL BODIES TO ADDRESS SRHR NEEDS IN THE REGION
In the face of legal, religious, societal, financial, security and geographical barriers to women’s and girls’ freedom to have full control over their bodies and to the provision of SRH services, local NGOs specialized in these areas are working to initiate and sustain positive change. Due to the nature of the SRHR field, NGOs adopt multi-sectoral approaches where access to education, social protection, health and law are intertwined in the implementation of their actions for the improvement of girls’ and women’s living conditions and the full exercise of their rights [54] .
Advocacy by local NGOs for governments
Their advocacy work with government institutions mainly calls for the establishment of a legal framework that protects women’s rights (including safe and legal abortion), as well as their physical and moral integrity with regard to SRH medical care, and that prohibits gender-based discrimination and violence. They work with parliamentarians and representatives of ministries responsible for health, education and women’s and girls’ issues to change the legal framework. This gives NGOs allies in government to take up their fight and support concrete legal progress in terms of SRHR . The main challenge is to achieve national ownership of SRHR issues. In the same perspective, NGOs demand that governments take up their responsibilities and commitments with regard to international and regional treaties upholding women’s rights that have been signed, with a view to respecting these rights and incorporating them into national legislation [55] . It is therefore essential for NGOs, governments and local political institutions to work together in order to « co-construct the response to SRHR needs on the ground and ensure the sustainability of projects by allowing local authorities to take over afterwards » [56] .
In some of the countries in our study, the government sometimes supports NGO projects. For example, in Niger, the National Assembly hosts the Nigerian Cell of Young Female Leaders (CNJFL) “Junior Parliament” project, which establishes a system of mentoring and leadership training between successful women and young girls at school [57] . In the DRC, the new government has almost 30% women. President Félix Tshisekedi spoke in favour of the promotion of women’s rights and mentioned the Maputo Protocol in his inaugural speech [58] . Furthermore, "the new government has put in place a programme of priority actions for the term of office, including family planning and the fight against gender-based violence. The Maputo Protocol is being implemented through a normative framework and a technical repository on women-centred comprehensive abortion care in the DRC. Thus, at the sub-region level, the DRC is progressively playing a leading role in SRHR, an influence that is reinforced by the presence of President Tshisekedi as the current chair of the African Union” [59] .
In Burkina Faso, champion of the “Bodily Autonomy and Sexual and Reproductive Health and Rights” action coalition within the framework of the Generation Equality Forum, the government stands out for its assertive and committed political discourse on SRHR. At the UN Commission on the Status of Women in 2021, the Minister of Health Charlemagne Ouédraogo reiterated Burkina Faso’s commitment to promote and guarantee women’s well-being and autonomy through free access to contraceptive and family planning services. He also made a progressive case for abortion and the importance of developing comprehensive sex education in schools to prepare future generations. The Minister of Health also emphasized the central role played by NGOs in governments’ strategies, saying that they should be responsible for monitoring the accountability of countries in terms of SRHR.
Advocacy by local NGOs for communities
Civil society organizations (CSOs) also carry out important advocacy work with communities through “community dialogue on SRHR to engage in discussions on the impacts of communities committing or not committing to the promotion of SRHR. These opportunities for interaction encourage intergenerational discussion, as well as discussions between women and men, i.e. groups that do not usually discuss sexual and reproductive health amongst themselves” [60] . When these NGOs reach out to communities, religious and community leaders are particularly targeted and made aware of the importance of women’s empowerment, girls’ education and the eradication of harmful practices such as FGM, underage and forced marriages. To do this, NGOs identify receptive leaders who will be listened to because of their influence and knowledge of the community, facilitating the transmission of information and the freeing of speech on certain sensitive SRHR issues. Indeed, "the voice of religious and community leaders matters so much that if they approve of something, the community accepts it. Religious leaders who are identified and won over to the cause then uphold the NGO’s discourse against child marriage, for example, and continue actions in the community after the NGO has left. They have the power to change behaviour within a community” [61] .
The strength of local NGOs lies in their ability to relay their awareness-raising message about SRHR through ambassadors in the communities, helping to create a network to fight misinformation and superstition. The intention is to engage all stakeholders in the community in order to provide them with the right information on SRHR and to include them in actions undertaken to promote SRHR. This strategy is all the more relevant as regular changes in political regimes disrupt any work carried out with political representatives. By engaging at the community level, continuity in NGO advocacy work is possible [62] .
Furthermore, "community ownership of SRHR is crucial as there are still zones where it is impossible to talk about SRHR and for it to be acknowledged that many adolescents are sexually active. Imams participate in many CSO networks and platforms at national and regional level and facilitate this advocacy work within communities and with the authorities. One example is the collaboration of the Ouagadougou partnership with the network of religious leaders in West Africa. There is a change in cultural acceptance of the right to contraception and medical abortion under certain conditions (rape, incest or danger to the mother). Progress is being made, albeit slowly. Moreover, the pressure and advocacy of youth movements is becoming so substantial that it cannot be ignored for long” [63] . The dynamism of young people’s demands for reliable information and access to SRHR services no longer allows communities to ignore these issues.
Thus, whether at the level of governments or civil society, progress is being made through a gradual opening of dialogue on SRHR. This must be continued and sustained. While « in the early 2010s, the subject of family planning was taboo, it is now being raised within the community and with policy makers » [64] . Advocacy by institutions such as the Ouagadougou Partnership, the African Union, the West African Health Organization and ECOWAS, is helping to revise national policies to incorporate new strategies for providing access to FP information and services to the entire population, including in hard-to-reach areas. Awareness of the importance of taking action on SRHR has thus been translated into action at regional, national and local levels. However, there are still many challenges in dealing with opposition and barriers to SRHR.
“Husband school" programmes implemented in all the countries studied aim to remove the barrier to information and access to sexual and reproductive health care. During these moments of exchange and awareness raising, men are involved and encouraged to acknowledge their responsibilities in issues relating to women’s rights, their autonomy and SRHR. Fertility concerns both men and women.
Although this may lead to an encouraging change in the acceptance of family planning discussions, as well as an increase in the number of women attending health centres [65] , the opinions of the women active in the NGOs interviewed [66] are nevertheless divided regarding the positive contribution of these programmes. While men are committed to addressing issues that were previously consciously passed over in silence, it gives them a platform where they can once again have the upper hand over women and their bodies. Indeed, in the countries surveyed, the majority of men control their partner’s sexuality, including the use of a method of contraception. However, it is primarily the responsibility of girls and women to freely make decisions that affect them. The Network of West African Young Feminists for Mali further argues that it is up to the whole population to « stop letting religious leaders and the government make decisions about SRHR so as not to allow a minority of men to mortgage young people’s futures » [67] .
Actions by local NGOs with and for youth
With regard to young people, NGOs are increasing their actions with and for them, which is a prerequisite for bringing about changes in mentalities and cultural and social practices, as well as for overturning old patterns in a region where people under the age of 25 represent more than 50% of the national population. Promoting female leadership and empowerment among young girls is a necessary condition for enabling new generations of women to make their own choices and express their needs in terms of SRHR. Their full emancipation depends on the realization of their potential, which must be communicated from the earliest age at school.
Among the actions carried out in schools to raise young people’s awareness of their SRHR and to open up dialogue on subjects considered taboo, the normalization of discussions about menstrual hygiene is for some NGOs, such as the CNJFL [68] , the keystone of their advocacy. In this sense, the CNJFL offers a safe space for discussion with young girls to fight against menstrual insecurity. Girls who menstruate are more likely to drop out of school because they cannot afford sanitary protection, because there are no separate latrines at school to give them privacy, and because the subject is taboo. Young boys are also involved through projects where they are trained in SRHR and girls’ empowerment issues and become 'ambassadors’. They are thus able to pass on this knowledge and become agents of change.
Providing comprehensive sexuality education (CSE) in schools is another area where these NGOs work with young people. Despite a lack of consensus on the name of this programme and the community and religious tensions it provokes, it is essential to include CSE in the training curriculum of education provided. NGOs stress the importance of educating young people about SRH in order to give them the knowledge to make their own choices and protect them from harmful and dangerous practices, such as unprotected sex, female genital mutilation, underage marriage and pregnancy.
Getting girls into school and keeping them there are therefore key elements of NGO advocacy against child and forced marriages and against women’s and girls’ dependence on men for their livelihoods. Local associations try to explain to families and communities, through community debates, that a girl who receives a full education then has the possibility of obtaining economic independence, thereby enabling the family to avoid taking decisions against the physical and moral integrity of their daughters due to a lack of financial resources [69] .
In a context in which many local languages exist in West and Central African countries, language is another limitation to the dissemination of information on SRHR within communities. The transmission of information in rural areas where different languages are spoken has therefore required translation work by NGOs through intermediaries in order to bridge language-based knowledge gaps and to achieve community ownership of the information [70] .
To address the lack of information about SRHR and to promote its accessibility and understanding, NGOs are also using radio and social media to spread knowledge more widely. These methods have been intensified as a result of the health crisis. Civil society organizations active in the promotion and defence of SRHR within the countries studied have once again demonstrated their resilience. NGOs have redoubled their innovative strategies to ensure continuity of services and information for the population. Social media have been used to spread online health and telemedicine programmes. For example, women and girls were able to self-administer subcutaneous injections of DMPA, a pregnancy prevention method, through telephone monitoring [71] .
Whether smartphone applications, social media or radio are used, the goal remains the same: to address the barriers created by the health crisis so that women and girls can continue to receive care [72] . After the closure of schools, social media proved to be the ideal platform for maintaining communication and providing information and advice to young people. In addition, it enables widespread access to care and better dissemination of information on SRHR. For remote areas without Internet access, community relays and mobile teams have been strengthened to bridge the digital divide [73] .
2. FRANCE’S STRATEGY FOR OFFICIAL DEVELOPMENT ASSISTANCE FOR SRHR IN WEST AND CENTRAL AFRICA
A. EVOLUTION OF THE INTEGRATION OF SRHR INTO FRENCH OFFICIAL DEVELOPMENT ASSISTANCE
To understand the changes in France’s official development assistance (ODA) policy regarding the integration of gender-related concepts, including SRHR, it is necessary to look at the first Stratégie genre et développement (Gender and Development Strategy) published by the government in 2007. In this document, France reports, for the first time, the adoption of a gender perspective in its external development assistance. Gender equality and women’s rights were included in France’s positions and programmes that it supports in international bodies, and access to SRH services was defined as an objective of France’s strategy. Following the evaluation of this document by the Observatoire de la parité entre les femmes et les hommes (Observatory of Parity between Women and Men) [74] , it was recommended that the government promote a cross-cutting approach [75] to gender issues in its development policies. To this end, « the training of agents, […] the provision of appropriate methodological tools and […] the reform of procedures for the appraisal, monitoring and evaluation of projects and programmes [76] » was recommended. The lack of resources and visibility is another element to be corrected.
In 2010, the French Muskoka Fund was established. Its mandate is to work towards the achievement of the Millennium Development Goals (MDGs) on reducing maternal and child mortality and increasing access to reproductive health care for nine countries in West and Central Africa (Benin, Burkina Faso, Chad, Côte d’Ivoire, Guinea, Mali, Niger, Senegal, Chad and Togo). The French Muskoka Fund is an innovative coordination mechanism between the World Health Organization (WHO), UN Women, the United Nations Population Fund (UNFPA) and the United Nations Children’s Fund (UNICEF) to strengthen the health systems of these countries and implement programmes in the areas of maternal, newborn, child and adolescent reproductive health (RMNCAH). France is the founder and main donor of this fund and has pledged 500 million euros from 2011 to 2015 through multilateral and bilateral channels [77] . More recently, France has been funding these various organizations with €10 million per year under the French Muskoka Fund from 2017 to 2022, the year in which the fund is due to close [78] . In 2011, the Ouagadougou Partnership was added to this commitment by France, which participates through the French Development Agency (AFD), one of the partnership’s donors. Since 2020, the AFD has been financing projects in West Africa, Benin, Mali, Niger, Burkina Faso, Côte d’Ivoire, Guinea, Senegal and Togo within the framework of the Ouagadougou Partnership [79] .
In 2014, under the five-year term of François Hollande, the Minister for Women’s Rights Najat Vallaud-Belkacem brought in the law no. 2014–873 in favour of real equality between women and men adopted on 4 August 2014. In the same year, the law n°2014–773 of 7 July on the orientation and programming of development and international solidarity policy gave a clear strategic direction to France’s development policies by including gender equality and considering gender as a cross-cutting issue in all sectors of French cooperation. This law affirms, among other things, the importance given to sexual and reproductive health by the French government. In the same year, the AFD adopted a cross-cutting intervention framework focused on gender and the reduction of gender inequalities, which takes a sectoral approach. The importance of « women’s and girls’ access to essential health information, commodities and services, with a focus on sexual health » [80] was thus highlighted.
Two years later, under Jean-Marc Ayrault’s government, a first report was devoted to SRHR in the document L’Action extérieure de la France sur les enjeux de population, de droits sexuels et reproductifs 2016–2020 proposed by Jean-Marc Ayrault, then Minister of Foreign Affairs and International Development, and André Vallini, Secretary of State in charge of Development and Francophonie. The three main areas are policy advocacy, reduction of harmful practices and family planning. This document is announced as a reference tool for French diplomacy, in which SRHR are seen as a key area of France’s political advocacy for gender equality and the defence of women’s rights. The approach of the government’s discourse was first to focus on the demographic dimension of SRHR and then to emphasize their importance for the empowerment of young women and equal opportunities between women and men. France’s role as a leading country within multilateral and regional bodies is underlined as a structuring axis of its political commitment to SRHR. In 2017, at the UN Commission on the Status of Women, the Minister for Families, Children and Women’s Rights, Laurence Rossignol, gave a speech committed to "the universal recognition of sexual and reproductive rights as an essential prerequisite for the empowerment of women” [81] . The renewal of this strategy for 2021–2024 is a crucial step in the government’s positioning on this issue and should enable it to strengthen its rights-based approach.
While France’s External Action on Population, Sexual and Reproductive Rights 2016–2020 presented the emergence of the Ministry of Europe and Foreign Affairs’ knowledge of SRHR, the strategy currently being developed aims to address all SRHR-related issues and to demonstrate an evolving understanding of the whole SRHR “package”, by taking into account, in particular, menstrual hygiene and the fight against toxic masculinity, issues that have so far received little attention [82] . The progress observed and to come concerning SRHR is in line with that identified in public debate and supported by civil society in France and which influences international support for these subjects [83] .
In recent years, France’s commitment to gender equality has been strengthened under the presidency of Emmanuel Macron, who has made this issue « the major cause of his five-year term » [84] . French Official development assistance policy, the tool for implementing this priority, underwent a change in 2018 following the meeting of the Interministerial Committee for International Cooperation and Development [85] . It is stated that ODA pursues, among other things, the achievement of the Sustainable Development Goals (SDGs) through the identification of sectoral, budgetary and geographical indicators. Since then, gender equality has been considered as « a guiding and cross-cutting principle of France’s external action » [86] in which a rights-based approach is prioritized. ODA is also planned to reach 0.55% of gross national income (GNI) for the period 2018–2022. To achieve this, financial commitments have been made to UN Women, UNFPA and the French Muskoka Fund [87] . ODA funding for gender equality will be identified via the « gender marker » established by the Development Assistance Committee (DAC) to ensure monitoring and accountability. In terms of geographical areas targeted by ODA, Africa is given particular attention, including the five countries in our study. Nevertheless, it should be stressed that the actions carried out in favour of SRH remain associated with objectives linked to demographic transition [88] , whereas the two approaches can be dissociated insofar as respect for individual rights is unconditional, independent of any public policy, health or demographic objective.
La Stratégie internationale de la France pour l’égalité entre les femmes et les hommes (France’s International Strategy for Equality between Women and Men 2018–2022) advocates a rights-based approach to gender mainstreaming in all of France’s external action. The funding targets presented aim to achieve « 50% of programmable bilateral ODA, by volume of funding, with the primary or significant objective of reducing gender inequality by 2022 (OECD markers 1 and 2) » [89] . In addition, « the AFD will have an absolute value minimum volume target for funding programmes marked 2, according to a progressive trajectory that will aim for an amount of 700 million euros per year in 2022 » [90] .

Source: “Handbook on the OECD-DAC Gender Equality Policy Marker”, OECD, December 2016.
Shortly afterwards, France announced the adoption of feminist diplomacy as part of the new impetus given to the country’s ODA. Feminist diplomacy was previously upheld in 2016 by Pascale Boistard, Secretary of State for Women’s Rights, who made a declaration relating to professional equality, parity and women’s rights, arguing for the positive implications of implementing diplomacy promoting gender equality and women’s rights in societies [91] .
France’s feminist diplomacy As a new political concept, only four countries claim to uphold it, these include Sweden, Canada, France and Mexico. Feminist diplomacy in France was introduced by the Minister of Foreign Affairs and Europe, Jean-Yves Le Drian, on 8 March 2018. It is based on the principles of including gender equality in France’s foreign policy strategy, which includes combating gender inequality, defending women’s rights, mobilizing human and financial resources to achieve this and the involvement of more women actors in international relations.France’s feminist diplomacy is characterized as “pragmatic and progressive” by the High Council for Equality. While the approach is broad, priority themes have been identified: sexual and reproductive rights, combating sexual and gender-based violence, girls’ education and women’s economic empowerment. The implementation of the strategy is mainly carried out through official development assistance.
The draft programming law on solidarity development and the fight against global inequalities, proposed in March 2021, is part of the new feminist diplomacy. This bill stipulates that 20% of bilateral ODA commitments must have gender equality as a primary objective. In this way, the concepts of gender equality and respect for women’s rights are integrated in a cross-cutting manner into all of France’s programmes and interventions. This law replaces the law of 7 July 2014 and provides for an increase in ODA to 0.55% of GNI by 2022 and then to 0.7% of GNI in 2025. The sub-Saharan African region is particularly concerned by this ODA review. Indeed, it is stated that the AFD « is placing increasing emphasis on the SRHR approach, the fight against female genital mutilation and population dynamics in Sub-Saharan Africa » [92] .
In the context of these various initiatives to promote gender equality in France’s external actions, ambassadors are key actors in the implementation of the government’s commitments and upholding the country’s discourse on rights and SRH issues. In order for foreign policy to reflect the commitments made by the government, ambassadors must promote and highlight the issues defined with the governments of their countries of residence, while taking into account their sensitivities in order to maintain an open dialogue and gradually make progress.
Following the Generation Equality Forum, which will close in early July 2021, the French Embassy will continue to « accompany and support initiatives taken on these themes with the aim of contributing to the mobilization of new funding to carry out Burkina Faso’s commitments made at the Generation Equality Forum », in conjunction with UN Women, which is at the forefront of the defence of women and girls with governments and civil society. In this regard, "Burkina Faso should benefit from additional funding from 2021 thanks to its return to the French Muskoka Fund, which aims to improve the health of women, newborns, children and adolescents in West and Central Africa” [93] .
On the international scene, France has asserted its willingness to uphold strong, committed political advocacy for gender equality and women’s right to have control over their own bodies. However, for several years, the international environment has been marked by a resurgence of conservatism and traditionalism championed in international bodies by a coalition of countries such as Saudi Arabia, Russia, Brazil and, more recently, by the United States under the presidency of Donald Trump, leading to a regression (or backlash) in women’s rights throughout the world [94] . The former US President waged a war on women’s rights, including SRHR, in multilateral bodies. In 2017, the Mexico City Policy, also known as the “global gag rule”, was reinstated by Donald Trump. « This rule prohibits the allocation of US federal funds to civil society organizations working abroad that provide abortion counselling or referrals, advocate for the decriminalization of voluntary termination of pregnancy, or expand available abortion services – even when the US does not fund these services itself” [95] . The consequences of this measure have been disastrous for funding for the health sector and for official development assistance dedicated to SRHR, resulting in considerable financial losses for SRH services. Following the US announcement, it was estimated that the NGOs concerned would suffer losses of $600 million [96] . To address this, a fund-raising campaign, She Decides , was launched in 2017. France announced its support by committing an additional €1.5 million to UNFPA and in 2018 the French government announced that it would »allocate an additional €10 million for SRHR concurrent with the 62nd session of the UN Commission on the Status of Women” [97] .
In April 2019, the US refused to vote for a UN resolution against sexual violence in armed conflict on the grounds that mentioning sexual and reproductive health was tantamount to supporting abortion [98] . Finally, in October 2020, US Secretary of State Mike Pompeo used the country’s influence to encourage around 30 governments to sign the Geneva Consensus Declaration [99] , which states that abortion is a matter of national law and not of international jurisdiction. The election of Joe Biden as President of the United States in 2021 was an opportunity to lift all of these measures attacking women’s rights.
In the face of increasing advocacy and heavy-handed decision-making by conservative and religious groups around the world, France has decided to react and intensify its advocacy on SRHR 3 at the UN Human Rights Council, the G7, the UN Commission on Population and Development, the UN General Assembly and the UN Commission on the Status of Women. In the mid-term accountability report on France’s External Action on Population, Sexual and Reproductive Rights 2016–2020, it mentions France’s initiative to draft “a communiqué endorsed by thirty-one UN Member States that regretted the failure of the negotiations and called for the recognition of sexual and reproductive rights, including voluntary termination of pregnancy, as full human rights” [100] .
The Generation Equality Forum, co-chaired by the French government, is an opportunity to create an action coalition committed to the defence of SRHR through the collaboration of multiple actors, such as governments, NGOs and companies. This configuration makes it possible to bypass the usual blockages that prevail within multilateral bodies with regard to women’s rights and in particular the issue of SRHR. It is also an opportunity to create synergy across the world in favour of the implementation of concrete initiatives for SRHR through dedicated funding over five years.
The Generation Equality Forum The Generation Equality Forum is organized by UN Women and co-chaired by France and Mexico.It is a global gathering for gender equality that puts civil society and all stakeholders at the heart of its actions. The forum is essentially in line with the same logic that made possible [twenty-six years ago] the decisive step forward represented by the adoption of the Beijing Platform for Action. This programme and its progress embody the power of activism, feminist solidarity and youth leadership to achieve truly transformative change in our societies.The Generation Equality Forum is a high point for the commitment of gender equality advocates from every sector of society (governments, civil society, the private sector, entrepreneurs, trade unions, artists, academics and influencers), which will initiate a global public debate on the need for urgent action and accountability for gender equality for all actors.(Source: https ://forum.generationequality.org/)
B. FRANCE’S FUNDING FOR SEXUAL AND REPRODUCTIVE HEALTH AND RIGHTS
The implementation of these multiple commitments and initiatives defined by France in favour of the defence of women’s rights and SRHR requires the allocation of funds. So, what is the current situation regarding France’s official development assistance (ODA) funding for SRHR in sub-Saharan Africa? The funding dedicated to SRHR by the French government will be presented in the most comprehensive but not exhaustive manner possible, due to the difficulty of tracing and identifying these funds.
Indeed, the report presented by the Ministry of Europe and Foreign Affairs in France’s International Strategy for Equality between Women and Men (2018–2022) notes the difficulty of summarizing all ODA data. The data is public, but the SRHR programmes, as we have seen, are cross-cutting, and can therefore be counted across different programmes, whether they concern health, education or the fight against discrimination. In addition, programme monitoring indicators are analytical in nature, whereas SRHR follow multiple objectives, which can therefore be counted several times.
This is compounded by the diversity of methodologies used to account for French ODA funding for SRHR. There is therefore a lack of precision in identifying and accounting for such funding. In addition, the diversity of accounting methodologies does not enable the comparison of figures corresponding to French ODA allocated to SRHR.
There can be no doubt that these technical difficulties in monitoring the programmes limit their understanding for external observers, partners in public action and, even more so, for citizens. In terms of accountability, it would be necessary to define a method, shared with all stakeholders (ministries, operators, associations, civil society, etc.) to cross-check information and provide assessments to verify that aid programmes are in line with the commitments made by France on the international scene, particularly when it acts as a champion for a major cause. The lack of visibility is indeed « a major challenge for the understanding and legitimacy of development, cooperation policies, and for enhancing aid effectiveness » [101] . In 2016, Family Planning, Equipop and Médecins du Monde published a joint position paper [102] about French funding for SRHR where they agreed that precise identification of such funding is complex. In 2020, the French Development Agency (AFD), in its evaluation of the French Muskoka commitment, demonstrated that "the heterogeneity of the purposes of the accountability periods, collection procedures and the indicators” [103] makes it difficult to analyse funding associated with this issue.
Methodologies for accounting for financial resources allocated to SRHR by France
Funding dedicated to SRHR is mostly aggregated and inserted into more general projects that have a cross-cutting aim, thus contributing to their lack of traceability. The earmarking of funding allocated to SRHR is therefore essential to identify precisely the resources dedicated to this issue. The system used to trace specific funds for Reproductive, Maternal, Newborn and Child Health (RMNCH) and its sub-components is the OECD DAC system. It identifies each sector by a code, for example 13020 for reproductive health care or 13030 for family planning. However, these accountability instruments must be deployed correctly, which is not always the case [104] .
The DAC methodology has been criticised for the excessive interpretation involved in classifying and assigning codes to an SRHR project, the difficulty of assigning a specific code to a project with multiple aspects and the difficulty of categorizing general budget support for SRH and family planning [105] .
According to the Muskoka accountability methodology, French disbursements are estimated at €437 million by 2022 out of the €500 million pledged in 2010 [106] . This methodology for recording expenditure for the French Muskoka Fund defines weighted rates for each international organization to which the G7 countries contribute financially.
Muskoka weighting rates applicable to multilateral institutions

Muskoka weighting rates applicable to bilateral commitments (project sectors)

Source: G8 2010, Methodology for Calculating Baselines and Commitments: G8 Member Spending on Maternal, Newborn and Child Health
The Muskoka accountability methodology is flawed in the way it is applied and difficult to understand. Indeed, the imputation percentages, or weighting rates, are not properly monitored and adapted since « this methodology specifies the application of a single rate per project, whereas projects have several different components » [107] . In addition to this, the application of indicators is subject to interpretation and suffers from a lack of knowledge on the part of the teams responsible for ODA reporting. The accounting of funding for SRHR is also affected by the reporting of financial commitments but not the disbursements of these funds. Finally, the cumbersome process of information flow between the multiple actors responsible for data collection and accountability monitoring fragments the methodology [108] .
In 2020, a new methodology was adopted called the « Muskoka 2 methodology ». This methodology uses some of the OECD Creditor Reporting System codes [109] but assigns different percentages to them. It allows an estimate of total ODA allocated to RMNCH to be obtained while also having the disaggregated amounts available for RMNCH, which was not possible with the old methodology.
Finally, there is another methodology used by Countdown 2030, a consortium of European NGOs working to promote human rights and investment in family planning. Their methodology is based on more precise indicators than the OECD for sexual and reproductive health and family planning. The three indicators used are: total contributions to UNFPA, multilateral funding for SRH/FP, and total « SRH/FP funding flows from partners to multilaterals + project funding to multilaterals + funding to international organizations / initiatives / research » [110] .
Countdown 2030 is based on data provided by the Ministry of Europe and Foreign Affairs. In general, these methodologies depend on the ability of donors to correctly report on funding disbursed and received according to the indicators and weighting rates used. However, as mentioned above, accounting for and identifying funding for this issue, which covers multiple areas, has proven to be complex. In addition, there is a need to follow the accountability methodology for commitments that will be made in the Generation Equality Forum and to involve all stakeholders – UN Women, governments and civil society.
French funding for SRHR since 2011
According to the mid-term accountability report of France’s External Action on Population, Sexual and Reproductive Rights 2016–2020, from 2011 to 2016, "France spent an average of more than 300 million euros annually on sexual and reproductive health and rights” [111] .
In the context of the G7 in 2010, the French government pledged to provide 500 million euros to fund women’s, children’s and adolescent’s health and the fight against maternal and child mortality over the period 2011–2015. This funding was distributed through the bilateral channel, mainly managed by the AFD, and the multilateral channel to the French Muskoka Fund, the Global Fund to Fight AIDS, Tuberculosis and Malaria and the Global Alliance for Vaccines and Immunization (GAVI).
The 2020 diagnosis of the French Muskoka Fund states that the financial resources mobilized by the French government are far from meeting needs on the ground and are not commensurate with France’s political commitments to maternal, newborn, child and adolescent reproductive health [112] .
Evolution of France’s funding for RMNCAH-N for the French Muskoka Fund
Bilateral channel | Multilateral channel | |
2011–2014 | € 18,000,000 per year | € 44,300,000 per year |
2015–2018 | € 10,000,000 per year | € 10,000,000 per year |
Source: Évaluation formative sur l’engagement français Muskoka (2010–2017) (Formative Evaluation of the French Muskoka Commitment), Technopolis, 2019.

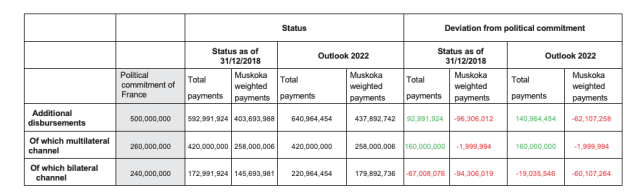
Source: MEAE/ DGM/ DPO and AFD data – Technopolis processing
NB: The data presented in this table shows the disbursements corresponding to commitments made between 2011 and 2015 by France (bilateral and multilateral channels). The amounts relating to the continuation of France’s Muskoka commitment after 2015 through the FSP to the FMF and the voluntary contribution to the FM are not included in this report.
France’s funding for SRHR is channelled through various platforms, such as UNFPA, the Global Fund to Fight AIDS, Tuberculosis and Malaria, and the AFD.
United Nations Population Fund (UNFPA)
The UNFPA is the UN agency responsible for development funds for sexual and reproductive health (SRH) issues. Its role is to combat maternal mortality and gender-based violence (GBV), as well as to address family planning needs. SRHR services cover the entire continuum of care: comprehensive sexuality education (CSE), access to SRH for youth and adolescents, voluntary family planning and maternal health care. In order to ensure accessibility to comprehensive SRHR services, France also provides financial support to UNFPA Supplies which delivers modern contraceptives. This commitment should be renewed in the framework of the Generation Equality Forum, as announced at the first phase of the Forum in Mexico City in March 2021.
French funding to UNFPA in dollars (2014–2019) | ||||||
Year | Main activities | Non-core activities | UNFPA Supplies | Emergencies | Other | Total |
2014 | 5,882,353 | 752,394 | - | - | - | 6,634,747 |
2015 | 3,947,871 | 623,583 | - | - | - | 4,571,454 |
2016 | 3,311,258 | 835,897 | - | - | - | 4,147,155 |
2017 | 597,117 | - | 1,074,114 | 530,786 | 3,976,436 | 6,178,453 |
2018 | 674,847 | 3,703,704 | - | 580,720 | - | 4,959,271 |
2019 | 1,251,422 | 4,183,448 | - | 556,174 | - | 5,991,044 |
Sources: Donor Rankings 2019, UNFPA.
Global Fund to Fight AIDS, Tuberculosis and Malaria
The Global Fund to Fight AIDS, Tuberculosis and Malaria channels the resources of the world’s private and public actors to invest strategically in programmes with the goal of ending these epidemics. However, actions under the Global Fund’s mandate also include SRHR issues in global health funding. Women and girls are particularly vulnerable to HIV, TB and malaria. According to the Global Fund’s official website, in "sub-Saharan Africa, more than 25% of infections affect [girls and young women], even though they represent only 10% of the population. Adolescent girls are more than twice as likely to be infected with HIV as adolescent boys” [113] . The Global Fund invests more than $4 billion per year.
The relatively small amounts of French funding for SRHR are justified by the large sums allocated to the Global Fund, a significant part of which is devoted to SRHR. In the document on France’s external action on population, sexual and reproductive rights issues for 2016–2020 , it is mentioned that "the Global Fund to Fight AIDS, Tuberculosis and Malaria devotes 41% of its budget to sexual and reproductive health services” [114] . However, according to the Muskoka 2 methodology, only 20% of Global Fund funding is dedicated to SRHR [115] .
It is important to clarify that this is not in any way to question the funding allocated to this fund – which is fundamental – but rather to encourage the government to be more precise in identifying funds for SRHR in general to enable better accounting.
France’s commitments and funding to the Global Fund (2014–2022)
Period | Commitment (€) | Contribution (€) |
2014–2016 | 1,080,000,000 | 1,026,000,000 |
2017–2019 | 1,080,000,000 | 1,004,400,000 |
2020–2022 | 1,296,000,000 | 266,370,000 |
Source: Government and Public Donors, The Global Fund.
Official development assistance via the French Development Agency
France’s official development assistance (ODA) funding in the sub-Saharan African region is in line with the SDGs set by the United Nations member states for 2030. France, which devoted 0.4% of its GNI to ODA in 2017, is gradually increasing its effort and is aiming for 0.7% in 2027. In 2019, €10.9 billion was spent on ODA, or 0.44% of GNI. In 2020, ODA was €12.4 billion or 0.53% of GNI [116] . For 2022, its commitment is 0.55%. With regard to the indicators guiding France’s ODA, 70% of it is directed towards sub-Saharan Africa and 41% to SRHR issues [117] .
According to the AFD’s Universal Registration Document, AFD projects dedicated to reproductive, maternal, newborn, child and adolescent health and nutrition (RMNCAH+N) amounted to 43 million euros in 2019 [118] . In the same year, following the G7 meeting chaired by France, France launched the Fonds de soutien aux organisations féministes (Support Fund for Feminist Organizations) initiative to finance gender equality projects run by feminist civil society organizations in France’s international cooperation and development partner countries.
The fund was endowed with 120 million euros for a period of three years starting in 2020 and favours an even distribution of the amounts allocated of 40 million euros per year. The management of three funding channels is co-supervised by the Ministry of Europe and Foreign Affairs and the AFD: AFD projects and calls for projects directed at women’s civil society organizations in partner countries, the AFD’s CSO initiatives mechanism for French CSOs and for the Solidarity Fund for Innovative Projects, Civil Societies, French-speaking countries and Human Development (FSPI)/Innovative Support Project for Civil Society and the Community of Actors (PISSCA) carried out by French embassies abroad for feminist CSOs in partner countries. This fund meets a geographical criterion, « projects must be at least 65% dedicated to the African continent, which meets the priorities of the French international cooperation agenda » [119] . For the French-speaking West Africa region, Equipop is part of a consortium of associations that work on the ground with local NGOs.
In 2020, five projects [120] with a total value of €35.5 million were launched for the first channel. Regarding calls for projects, 15 million euros was allocated to a consortium of associations, with the goal that 50% be targeted at SRHR issues. SRHR were also taken into account: in projects such as the Sahel Gender Fund, with 5.5 million euros of funding, and the call for projects to improve SRHR for adolescents and young people in Senegal, supported by a consortium of associations, with 8 million euros. As for the second channel [121] , ten projects in favour of SRHR, the fight against violence, economic empowerment, social and political leadership were approved for an amount of 5.279 million euros.
The originality of this fund is characterized by three major changes [122] . First of all, the AFD works directly with feminist NGOs. The challenge was also to propose modest amounts and therefore adapted to the capacities of grassroots feminist CSOs. Finally, there is the issue of real co-construction work with the NGOs in order to understand their needs and their ecosystem. In addition, in the case of NGO consortia, the Fund plays the role of intermediary with a view to capacity building.
This approach to funding local NGOs is all the more relevant as it meets the needs of the local ecosystem and works as closely as possible with local populations [123] . Funding feminist associations enables a direct connection with civil society. In addition, donors cannot focus solely on intervention funding, for example the establishment of a clinic for girls’ access to family planning. It is important to support actions that have a long-term impact, such as staff training, and that engage stakeholders on the ground to ensure community ownership [124] .
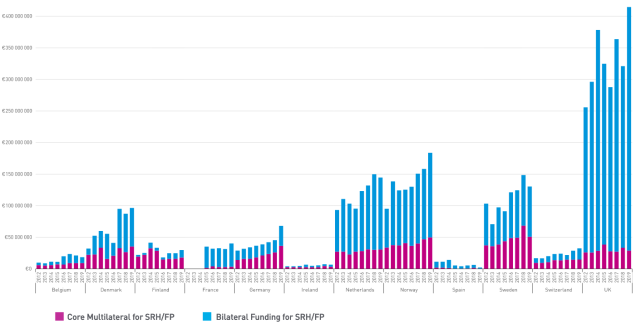
Source : European donor support to sexual & reproductive health & family planning. Trends analysis 2019–2020, Countdown 2030 Europe, janvier 2021.
Based on data collected by the OECD’s Creditor Reporting System, using the DAC codes presented earlier, France’s bilateral official aid in dollars for 2019 to health and SRHR is shown below, compared to that of other donors.
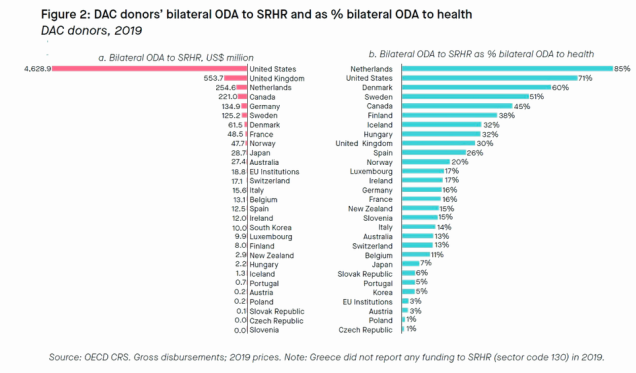
With regard to the multilateral channel, France donated 13,709,775 euros to programmes in favour of sexual and reproductive health and family planning in 2019 according to the Countdown 2030 [125] methodology. The Countdown 2030 Europe report also provides the total amount of funding for SRH/FP including funding for international organizations and initiatives, and the research sector, excluding the bilateral channel, which amounted to €40,358,775 [126] .
Comparison of national funding allocated to SRHR
For decades, France has been one of the leading countries committed to giving a significant voice to SRHR within international bodies. However, the funding allocated to SRHR by France shows a mismatch between its political and financial commitments, even though gender equality has been defined as the major cause of the five-year period by the President of the Republic. For this reason, the impact of French advocacy is reduced in comparison with the action of its international partners who grant more funding to this sector.
Funding | Funding | Funding | |
for SRHR 2016 | for SRHR 2017 | for SRHR 2018 | |
(millions $) | (millions $) | (millions $) | |
Germany | 323.111 | 310.788 | 313.281 |
Canada | 193.908 | 255.367 | 300.851 |
France | 181.605 | 193.369 | 197.566 |
Netherlands | 297.534 | 261.904 | 310.619 |
United Kingdom | 671.191 | 794.803 | 808.27 |
Sweden | 215.1 | 230.648 | 242.977 |
Source: Delivering Report 2020, European Parliament Forum for Sexual and Reproductive Rights.
It is therefore necessary to increase France’s funding by committing more resources per year for the period 2021–2026 as part of the new strategy on population and SRHR issues. A posture that would address the long-term effects of the withdrawal of funding for SRHR by the US through the reinstatement of the Global Gag Rule under former President Donald Trump, as well as the attacks on SRHR around the world that have been accentuated with the Covid-19 health crisis since 2020.
Impact of Covid-19 on funding for SRHR
Due to the Covid-19 health crisis, there are many concerns about funding for SRHR.
Due to the health crisis linked to Covid-19, the Equality Generation Forum will not be able to take place on a totally face-to-face basis as originally planned. The virtual configuration of the event is likely to have significant consequences on the funds mobilized for the Forum’s various causes, including SRHR. The organizations involved in the funding of this issue, as well as the beneficiaries of the grants, nevertheless hope that the Forum will have the expected mobilizing effect.
With regard to funding, Covid-19 exacerbated shortcomings in this area: women’s rights to control their own bodies were more than ever threatened with access to SRHR-related care being considered non-essential and therefore reduced. Like the withdrawal of US funding for SRHR, the coronavirus crisis has highlighted the dependence of recipient countries on external health assistance and the difficulties of these countries to sustain and meet the demand for SRH care. In addition, the disruption of care in the countries covered by our report reflects the lack of integration of SRHR programmes into local systems.
During the epidemic, aid programmes faced new obstacles, target populations were harder to reach, and local authorities were mobilized for Covid-19 emergencies. Projects that were in the process of being launched were suspended and their budgets reallocated to the crisis response. « Donors’ efforts seem to be focused on Covid-19, with investments in other more structural issues being put on the back burner » [127] . In this sense, the pandemic risks undermining and reversing the progress that had been made in SRHR for populations in sub-Saharan Africa. It also serves as a reminder of the need to further increase support for resilient health systems to promote sexual and reproductive health. Investment in health must be a long-term process; it takes years to see significant changes, especially when it comes to women’s rights. The repercussions of a reduction or removal of support for SRHR would therefore be disastrous for the rights of women and girls to have control over their own bodies.
According to the report conducted by Equipop [128] with its partners in Benin, Burkina Faso, Côte d’Ivoire, Guinea, Mali, Niger and Senegal, the financial support provided by donor countries has been subject to two different approaches during the pandemic. Some local NGOs report a « flexibility in adapting activities, reporting deadlines or extending projects » [129] while others revealed neglect or even abandonment by their donors. However, « the attitude of donors and their ability to understand ‘on the ground’ issues strongly affect the ability of associations to remain active and provide relevant responses to the sectors of the community who need them » [130] . The approach of imposing the achievement of pre-defined results in order to obtain funding is not appropriate in the case of a crisis where actions need to be reassessed. This is why it is essential to focus on the quality, not the quantity, of the actions carried out [131] , as well as on the sustainability of funding and strategies to respond to the coronavirus that have a major impact on the rights of women and girls. The health crisis will therefore have highlighted the need for countries to re-examine their ODA funding systems for SRHR to meet needs on the ground.
3. Recommendations
In light of the observations made on French funding for SRHR and on the basis of the interviews conducted with various political, institutional, economic and societal actors involved in this issue in sub-Saharan Africa, we propose to present some recommendations in line with the priorities in the field.
1. INCREASE FRENCH FUNDING FOR SRHR
France’s efforts in terms of funding mobilized for SRHR must be recognized. On the other hand, it is crucial to provide greater funding for the entire SRHR care package to be able to respond to the needs on the ground in a context of regression of women’s rights, accentuated by the health crisis and the gradual disengagement of some donors. France, as a champion among the partners of the bodily autonomy and SRHR action coalition at the Generation Equality Forum, would be all the more credible on the international stage. The government’s new strategy on external action on population and sexual and reproductive rights issues will be crucial in this regard.
2. COVER THE FULL RANGE OF SRHR ISSUES TO MEET NEEDS ON THE GROUND: A PRIORITY FOR RESPECTING WOMEN AND GIRLS’ FUNDAMENTAL RIGHTS
The priorities for SRHR are similar across the countries studied in this report: to encourage the enrolment of girls in school, to promote comprehensive sexuality education (CSE), to promote access to contraceptive methods and safe and legal abortion, to combat gender-based violence (GBV), female genital mutilation (FGM) and to support the empowerment and leadership of girls and women. These are all key areas to be targeted to enable women and girls to have the means to take charge of their own as a condition for their emancipation and as fundamental, universal human rights.
3. SIMPLIFY THE PROCESS OF IDENTIFYING AND ACCOUNTING FOR FUNDING FOR SRHR
The aim here is to make funding for SRHR more transparent and easier to understand, whether through the bilateral or multilateral channel. Accountability methodologies, scoring processes and data comparability need to be simplified to allow for better monitoring of French grants for SRHR. The earmarking of funding needs to be applied more clearly to facilitate the analysis of French funding for SRHR. In addition, there is a need to follow the accountability methodology for commitments that will be made in the Generation Equality Forum and to involve all stakeholders – UN Women, governments and civil society.
4. FAVOUR THE FUNDING OF PROJECTS WITH A LONG TIMEFRAME
In order to achieve a sustainable improvement in SRHR indicators, it is necessary to invest in youth, civil society organizations, medical personnel and to continue to advocate to political representatives on SRHR issues. This investment must value the transfer of knowledge and local ownership of knowledge and skills to ensure continuous transformation in communities. It is also essential to maintain funding for projects that operate on a long term basis and to minimize short-lived projects or the discontinuation of commitments in order to generate significant, sustainable gains. Extending France’s financial commitments to initiatives such as the French Muskoka Fund, the Ouagadougou Partnership and the Support Fund for Feminist Organizations would help sustain the progress made in sub-Saharan Africa.
5. ADAPT FUNDING ELIGIBILITY PROCEDURES FOR LOCAL AND FEMINIST NGOs
The eligibility criteria for funding for young associations would benefit from being made more flexible to allow a greater number of NGOs, and especially a greater diversity of organizations, to be eligible for grants. Smaller organizations struggle to receive grants due to monitoring and evaluation requirements that are not suited to the human resources funded. These NGOs are essential in remote areas where health services are scarce.
6. INVEST IN THE POTENTIAL OF YOUTH
France’s ODA to target countries should be more oriented towards funding strategies for local and feminist NGOs that work for and with young people to reverse the SRHR trend. Representing half of the population in the target countries, there is an urgent need for technical and financial support for youth to meet the needs for SRHR services and information. While donors were previously reluctant to fund youth-led NGOs because of their lack of experience and inability to absorb the funds they received, these organizations were resilient and took concrete action during the pandemic [132] .
ANNEXES
1. Contributions
Demographic transition, status and trends in five sub-saharan african countries
Hervé Le Bras (EHESS/INED) 21/04/2021
Hervé Le Bras is a demographer and historian, director of studies at EHESS and director of research emeritus at the National Institute of Demographic Studies (INED).
The five countries that are the subject of this study are all located in sub-Saharan Africa, and more precisely between the two tropics. This region is the last in the world to experience strong population growth. Of the 81 million people added to the world’s population between 2019 and 2020, 27 million were in intertropical Africa, accounting for one-third of the global increase, while less than 13% of all humans live there. According to the average projection of the United Nations Population Division, this same area can be expected to concentrate three quarters of global growth in 2050.
Whichever way you look at the demographic situation in the five countries that are representative of their region, the figures are completely out of line with the world average (for details, see table 1 in below). The annual population growth of each of the others is higher than that of any country on any other continent: 2.8% in Senegal, 2.9% in Burkina Faso, 3% in Mali, 3.2% in the Democratic Republic of Congo (DRC), 3.8% in Niger (i.e. a doubling every age 18 years). Between 1950 and 2020, the population of Senegal increased sevenfold, that of Mali and Burkina fivefold, the DRC sevenfold and Niger ninefold.
These multipliers will increase further according to the average UN projection for 2050. By then, the population is expected to increase to 33 million in Senegal, 43 million in both Mali and Burkina Faso, 65 million in Niger and 195 million in the DRC. Another picture of the scale of change that could occur in a century is that between 1950 and 2050, the population of Niger will have increased by a factor of 25 and that of the DRC by a factor of 16. Such upheavals are caused by high fertility, while infant and child mortality, which until recently had reduced growth, has become quite low, with at least 90% of newborns reaching adulthood.
The intermediate components of fertility in the five countries
The term « intermediate components » [133] characterizes fertility patterns, before looking for deeper causes. The total fertility rate, often referred to as the average number of children per woman, is very high in all five countries. While the world average has fallen to 2.5 children per woman, it is 5 in Burkina, 6 in Mali and the DRC, and 7 in Niger (the world record) [134] .
Three intermediate components are sufficient to account for the pattern of age-specific fertility and its overall level: the age at which a woman enters into a union, the prevalence of contraception and the duration of breastfeeding. The figure below shows that the higher the fertility, the earlier the age at which women start having children. According to the survey data, the first birth takes place when the mother is 21.9 years-old in Senegal and 20 years-old in DRC. In contrast, French mothers are on average 28 years-old when they have their first child. The second component, the frequency of contraception, plays the most important role. It is not used very often. Surveys estimate that it is used by about 20% of women at any given time in Mali, Senegal, Niger and Burkina. Condoms are hardly ever used. The pill (4% of users), douching and implants are the most common (7 to 8%) [135] .
Fertility rate by age (2012 – 2020)

The third component, the interval between successive births, is often ignored because it has traditionally been of little importance in Europe.
In Africa and part of Asia, on the contrary, long breastfeeding has long kept fertility in balance with mortality. In populations that have retained traditional practices, such as the Bochimanes in the Kalahari, who only wean their children after 30 to 36 months, this keeps fertility at around 4.5 children per woman. Indeed, during breastfeeding, women are less fertile or even avoid sexual intercourse. The advent of European methods of feeding children has resulted in shorter birth intervals. This has been followed by an increase in fertility. It could be said that the main obstacle to birth control was Nestlé powdered milk [136] . Indeed, in all five countries, fertility increased from the 1970s onwards, peaking in the early 1980s, and then beginning to decline. The benchmark for measuring the current fertility decline is therefore this maximum, since breastfeeding practices have not changed since then. For example, in Burkina Faso, fertility rose from 6.1 children per woman in the 1950s to 7.2 in the early 1980s and is now down to 5.2. The difference of two children is not negligible. The same is true in Senegal where, after peaking at 7.3 children, the index is now 4.7, halfway to the replacement rate of 2.1. For other countries, the decline was smaller: 6.8 to 6 in the DRC, 7.9 to 7 in Niger. Social, political and economic conditions, and thus the underlying determinants of fertility, vary considerably from country to country.
Social and political fertility factors in sub-saharan Africa
Three factors contribute to high fertility: early marriage, which we have just seen has an effect on first births, urban residence and education.
Urban fertility, rural fertility
The difference in fertility between urban and rural areas averages two children per woman in Senegal [137] , DRC [138] and Mali [139] , and three children in Burkina Faso [140] . The gap is even wider in the capital cities. For example, in Kinshasa, the fertility rate is 4.2, in towns it is 5.4 and in rural areas 7.3. There are several reasons for this: women attend school longer and in greater proportions, there is less societal pressure, and the adoption of the western lifestyle, with a smaller family, is more widespread. However, this is still a long way from the fertility levels observed in countries outside Africa. With an average of 4.9 children, for example, Malian women living in towns are still far ahead of countries on other continents, in both urban and rural areas. The total fertility rate is currently 2.2 in India and 1.7 in Brazil and China.
Education
The relationship between fertility and educational attainment is almost universal. Since the 1980s, global fertility surveys have shown that fertility begins to decline when women have completed a few years of secondary education. The fertility rate of those that graduated from high school was half that of women who had not received any secondary education. In contrast, primary education had little impact. However, secondary school enrolment ratios remain modest in the countries studied. Homogeneous data is available from UNESCO for five of them (Table 2) but only a rough estimate, combining both sexes, for the DRC. Senegal is the most advanced with 39% of women of secondary school age enrolled. This is followed by Burkina Faso with 32% and Mali with 27%. The furthest behind is Niger (17%). In DRC, only the rate for both sexes (27%) is known, and even this not very precisely. The hierarchy observed is fairly similar to that for fertility rates. The proportion of girls in primary education is significantly higher, but still far from 100%. Senegal and Burkina Faso again come closest (81% and 78% respectively). In these two countries, there is also a phenomenon that has become widespread in developed countries: women complete more studies than men.
At the other end of the educational spectrum, a significant proportion of the population remains illiterate. UNESCO estimated the number of illiterate people aged 15 to 24 in 2018 [141] . Relative to the total as reported by the UN, the following values were obtained in four countries: 30% in Senegal, 40% in Burkina and Mali, 55% in Niger. Again, DRC statistics on this issue are erratic. These values, which are difficult to compare precisely with gross enrolment ratios, do, however, confirm the hierarchy of fertility levels.
Why does education play such a role in reducing fertility? A West African anthropologist, John Caldwell, has provided a convincing explanation [142] . In traditional society, children are quickly profitable, because they can replace adults in the carrying out of simple tasks such as herding small livestock or helping their mother to sell products in the market. This is why education is often unwelcome in rural areas. There is also a biological fact. As they continue their secondary education, girls reach fertile age and must guard against conception if they wish to complete it, as births outside marital union are generally frowned upon, particularly in countries where Islam dominates. They therefore acquire some practice in reproductive control, either through abstinence or through traditional or modern contraceptive procedures.
Early marriages
The figures on age-specific fertility rates shows how early births occur in each of the five countries. This is due to the youthfulness of the women at the time of their first marriage. Three quarters of Nigerian women are married before the age of 18; this is the case for 50% of Malian and Burkina Faso women, 37% of Congolese women and of 30% of Senegalese women. Here again, the relationship with total fertility is clear. The average age of women at the time of their first marriage is 20.3 years in Senegal and 19.5 in Burkina Faso. In Mali, the median age is 17.8 years, which means that before the age of 18, more than half are already married, and confirms the first figures on the frequency of marriages before this age. In towns, marriage takes place an average of two years later. Thus, in Senegal, urban women are 22.5 years old on average at the time of marriage.
A detailed survey of adolescent marriages in Niger [143] gives the age distribution of adolescent girls and their husbands. 17% are 15 years-old or younger. Their husbands are significantly older, with 32% aged between 25 and 29, and 21% over 30. The median age difference between spouses is seven years. Such imbalances suggest that the man has all the power in the couple, which is often referred to as patriarchy. We will see later that the situation is more subtle, especially as 94% of the survey was conducted among rural households.
Factors explaining fertility levels
Some factors are overestimated, others downplayed or ignored. They range from anthropological to political.
Information
African populations are often seen as uninformed. It is not so much the quality of the information that matters, but rather that the means of obtaining information are numerous and have developed rapidly. This is known from the Multiple Indicator Cluster Surveys conducted in the five countries in 2012, 2013 or 2018 depending on the country.
Table 3 shows the percentage ownership of a radio, television and mobile phones and the year of data collection for the five countries covered by the surveys. By 2018, 97% of households in Senegal owned at least one mobile phone, both in urban and rural areas. 72% in Mali on the same date. In 2013, the figure was only 40% in the DRC, and in 2012, 59% in Burkina Faso and 50% in Niger [144] . By comparison, it can be estimated that by 2020, the ownership rate will be at least 80% in all countries (and almost 100% in Senegal). Households also often have a radio (66 % in Senegal, 68% in Burkina Faso, 52 % in Niger, 50% in Mali, and 43 % in the DRC). Only televisions are rarer, owned by about 15% of households.
Polygamy
Polygamy is quite widely practised in all five countries. Table 5 shows the proportion of women and men aged 15–49 living in polygamous unions. Burkina Faso leads with 42% of women living with co-wives, while the DRC is in last place, with 22%. The proportion is also quite high in the other three countries (32% to 37%). Proportionally, men are less likely to live in polygamous unions (from 10% to 22% depending on the country). Polygamy is decreasing, but slowly. In Niger, between 2006 and 2012, it decreased by two points. In Burkina Faso, for which the data is older, it affected 45% of women in 1987, 42% in 2001 and 42% in 2012. The proportion of women living in polygamy also increases rapidly with age, sometimes exceeding 50% (57% in Burkina Faso at 45–49 years).
To what extent does polygamy affect fertility trends? First, the idea that women living with polygamous husbands are significantly less fertile than monogamous ones must be rejected. In Senegal, where it was possible to calculate fertility according to the nature of the household in the late 1990s, monogamous women produced an average of 7.4 children, first wives 6.9, second wives 6.6 and subsequent wives 6 children, i.e. minimal differences [145] . Rather, maintaining polygamy means maintaining traditional family structures, which are conducive to high fertility. When couples are asked how many children they would like to have or what the ideal number of children in a household is, they usually give relatively high numbers.
Ideal and desired number of children
Two misconceptions have long circulated in this regard. One was that Africans were not able to control their fertility, the other, that men wanted a large family, but women did not. Surveys have put an end to these platitudes. As the five countries have similar features, only the two cases from each end of the spectrum will be given, that of the DRC in 2013 and Senegal in 2018. For a Senegalese woman, on average, the ideal family size is 5.4 children and 5.9 if living with a partner. In the DRC, these figures were 6.1 and 6.6 children respectively. The gap between what is considered ideal and reality is small: 0.7 more children ideally in Senegal, 0.5 in DRC [146] . One could think that having many children is rationalized by considering it to be normal. This is not what is shown in the details by age and number of children already born. Women aged 20–24 give an ideal of 5.1 children in Senegal and 5.7 in DRC. In the same country, 63% of those who already have 5 children want to have more than 6 (52% in Senegal).
For men, the ideal number of children is higher than that cited by women, but the difference is small: 7 children on average for Congolese men (6.1 for Congolese women), 6.5 for Senegalese men (5.4 for Senegalese women). One can put the difference down to polygamy. Logically, polygamists should declare a larger number of children as ideal. Indeed, it may be that the polygamy model encourages monogamists to aspire to a high number of children. Returning to John Caldwell’s explanation, both men and women take advantage of a child labour force. The anthropologist adds another element: each child represents an opportunity, however small, to succeed, for example to be called to assist a successful relative in a town.
In addition to the ideal number of children, which concerns the image that people have of society, researchers asked in all five countries the question of the number of children they personally wanted. The results are close to those of the ideal number: 5.7 in DRC compared to 6.6 actually observed at the time, 4 compared to 4.4 in Senegal (and in 2012, 4.6 compared to 5.3 observed). The values calculated in Burkina Faso, Niger and Mali fall between those of Senegal and the DRC. Consistent with these results, the reported number of unwanted births is very low (4.8% in DRC, 2.1% in Senegal).
There is also a great deal of consistency between the ideal numbers and the observed numbers when the figures are examined in more detail. For example, in the DRC, the ideal numbers are 5.2 in the city and 6.7 in the rural areas, 7.2 for women with no education, 6.7 if they attended primary school, 5.4 if they went to secondary school and 4.3 if they attended university.
Family size
Fertility is high in the countries under consideration because parents want to have a lot of children. In poor countries, family plays an essential role. It serves as social insurance when less than 5% of the population are covered by the government. It allows sociability to flourish. The larger the family, the better suited it is to these roles. The economist Gary S. Becker has contrasted this way of life with that of the developed countries in the form of the dilemma of quantity (of children) versus their quality, i.e. their level of education [147] . Other elements must also be taken into account in the composition of African families in the five countries such as polygamy, age gaps between spouses, the extended role of relatives, and the early marriage of girls, for example.
The survey Child Marriage, Fertility, and Family Planning in Niger conducted by the Promundo Group interviewed 1,200 married women under the age of 20. To the question of who had decided they should get married, 29% of young women said that they had made the decision, 53% that it was a joint decision with their future husband, 9% that their family decided, and 7% that it was their husband’s family. 13.5% of respondents were co-wives. The survey report states: " Polygamy is so accepted that women can be shamed for not having co-wives” [148] . Concerning the issue of relationships between spouses, 94% said that they often discuss problems with their husbands, and 97% that their husbands love and appreciate them.
However, this idyllic picture has a flip side. 90% of decisions are made by the husband and there is a strict separation of duties: for example, 66% of the women interviewed felt that they would be shamed in their village if their husband cooked or cleaned.
It should be noted that the survey was conducted in a rural area and that 45% of the adolescent girls had not been to school. Also, as shown in the examples above, change results from moving to towns and studying.
Political unrest
A new obstacle to change has arisen recently in all the countries concerned, except Senegal. Terrorist groups have expanded, or civil unrest has broken out. In Mali and Burkina Faso, pressure from groups affiliated with Al-Qaeda or Islamic State groups is wreaking havoc over ever-widening areas. In southern Niger, Boko Haram is stepping up its pressure by attacking villages. Serious and recurrent unrest continues in the DRC. How is this related to high fertility rates, one might ask. Unfortunately, the two would appear to be related. The other countries in the region with high fertility rates, Somalia and Burundi, are also experiencing serious unrest. On another continent, just next to Africa, Yemen, where civil war is raging, has the highest fertility rate in the whole all Asia.
A new feature of these conflicts is their anti-feminist ideology, which manifests itself through a regression in women’s rights, notably through the destruction of schools and the abduction of young women, often to provide wives for terrorists [149] . Outside Africa, the Taliban and the Islamic State in Mosul have led the way. Such movements are supported by some sections of the population who reject the Western
Conclusion
Fertility has evolved at the pace of the factors that determine it, and therefore quite slowly, as can be seen in the following table. It can be said that these countries are undergoing a very slow transition [150] .
Country | Date of fertility maximum | Level 1 fertility rate maximum | Fertility 2020 | Decrease in fertility |
DRC | 1990 | 6,8 | 6 | –0,8 |
Burkina Faso | 1990 | 7 | 5,2 | –1,8 |
Mali | 1980 | 7,2 | 6,4 | –0,8 |
Niger | 1980 | 7,9 | 7 | –0,9 |
Senegal | 1975 | 7,3 | 4,7 | –2,6 |
It can be calculated that the increase in the proportion of the population living in urban areas and advances in secondary education alone account for the decline in fertility in each of the five countries and will continue to have an influence in this regard in the coming years. This also means that there has been no change in the family way of life in rural areas. In town, a new family organization is created, in between the western model and the traditional local model. Efforts should therefore focus on secondary education for girls and on modernizing agriculture, which will accentuate urbanization by mobilizing a smaller agricultural workforce.
Detailed analysis shows that differences in the size of the decline reflect the differences between countries. Senegal, which has the lowest fertility of the five countries studied, is experiencing significant growth in secondary education and urbanization. Burkina Faso is second because of its school enrolment campaigns. The other three countries remain at lower levels. Their poverty and the disorganization as a result of the unrest they are experiencing limits the possibilities to increase secondary education capacity and modernize agriculture.
These remarks serve to emphasise the enormous diversity between the five countries. First, between the four in the Sahel and the one in equatorial Africa, whose physical environment is radically different. In the Sahel, agriculture is subject to major climate variations and the soil is relatively poor. In Niger, for example, the coverage of cereal consumption went from 112% in 2014 to 88% in 2017 and 108% in 2018. The DRC, with 40 inhabitants per square kilometre, on the other hand, has abundant water resources and can cope with a significant increase in its population.
Within these two groups of countries, the differences are not only in education, urbanization and fertility, but also in customs. To give an example, 21% of women have been circumcised in Senegal, 58% in Burkina Faso and 86% in Mali, but almost none in the DRC. The acceptance of this practice follows the same pattern. In addition, each of the five countries is far from homogeneous. Provincial differences often reach the same order of magnitude as differences between countries. In Mali, for example, 59% of men in the prefecture of Kidal are literate, but only 38% in the prefecture of Sikasso; only 3% of women in Kidal use modern contraception, compared to 19% in Sikasso. 46% of women under 20 have already had a child in the province of Timbuktu, compared to 28% in the province of Segou. The quality of the statistics must often be taken with a pinch of salt. Policies addressing women and fertility must therefore not only be calibrated by country, but also within countries, by region.
Let us conclude with a final point that is of great importance for the five countries: climate change. All of them are likely to be violently affected, both because of the already very high temperatures and because of the variations in rainfall. However, these countries are not responsible for the increase in CO 2 in the atmosphere, because their emissions are so low. The average person in the DRC emits 0.03 tons of CO 2 , in Niger 0.10, in Mali and Burkina Faso 0.18, and in Senegal 0.73. By comparison, the average American emits 15.5 tons. A doubling of the population in all five countries at their current rate of emissions would produce an additional 24.8 million tons of CO 2 , equivalent to what 1.6 million Americans currently emit. The bitterness , to put it mildly, of the five countries with regard to responsibility for the climate crisis, is understandable, as they risk paying the consequences of the industrialization of developed and emerging countries.
Tables
Table 1 : Demographic data
Country | Fertility | Population in 2020 | Population in 2050 | Rate of growth | Population in 1950 | P2020/ P2050 | P2050/ P1950 |
World | 2,5 | 7 800 | 9 700 | 1,1 % | 3 100 | 3,1 | 3,9 |
Senegal | 4,7 | 16,7 | 33,2 | 2,8 % | 6,7 | 6,7 | 13,3 |
Mali | 5,9 | 20,3 | 43,6 | 3 % | 4,9 | 4,9 | 9,3 |
Burkina Faso | 5,2 | 20,9 | 43,4 | 2,9 % | 4,9 | 4,9 | 10,1 |
Niger | 7 | 24,2 | 65,6 | 3,8 % | 9,3 | 9,3 | 25,2 |
DRC | 6 | 89,6 | 194,4 | 3,2 % | 7,3 | 7,3 | 15,9 |
Fertility: average number of children per woman. Population: in millions.
Table 2 : School enrollment ratios
Primary | Secondary | Illiteracy (15–24 years old) | |||
Country | Boys | Girls | Boys | Girls | |
Burkina Faso | 80 | 78 | 30 | 32 | 40 |
DRC | ** | ** | 27 | ** | |
Mali | 62 | 56 | 33 | 27 | 41 |
Niger | 69 | 58 | 23 | 17 | 54 |
Senegal | 72 | 81 | 36 | 39 | 29 |
Table 3 : Household media
Country | With radio | With TV | With laptop |
DRC (2013) | 43 | 15 | 40 |
Mali (2018) | 50 | 40 | 72 |
Senegal (2018) | 66 | 61 | 97 |
Burkina Faso (2012) | 68 | 16 | 59 |
Niger (2012) | 52 | 12 | 50 |
Table 4 : Fertility
Country | Fertility rate 15–19 years-old | Married before 18 years-old | Contraception 15–49 years-old |
Burkina Faso | 0,132 | 52 | 29 |
DRC | 0,138 | 37 | 22 |
Mali | 0,164 | 54 | 17 |
Niger | 0,154 | 76 | 16 |
Senegal | 0,068 | 29 | 22 |
Table 5 : Frequency of polygamie (% 15–49 years-old)
Country | Women | Men |
Senegal | 32 | 10 |
Burkina Faso | 42 | 22 |
DRC | 22 | 15 |
Niger | 36 | 21 |
Mali | 37 | 19 |
Regional situation in sub-saharan Africa
Irmine Ayihounton is a member of the West African Young Feminists Network in Benin. The Young Feminists Network of West Africa brings together feminist activists from French-speaking West Africa who present the views of girls and women to decision-making bodies at local, regional, national and international levels.
How would you describe the situation in your country regarding women’s access to the right to sexual and reproductive health? Can you tell us about the actions you are carrying out in this field?
The Maputo Protocol [151] is currently one of the key documents used to discuss women’s rights in Africa. This protocol states that women’s health rights, including sexual and reproductive health (SRH), include: control over fertility; decision-making power in matters of childbearing; free choice of contraceptive methods; information and protection against sexually transmitted infections (STIs); and education on family Plan (FP). However, in West Africa, the situation for women is still very unsatisfactory. In 2019, according to data provided by the Guttmacher Institute [152] , 33 million women of reproductive age want to avoid pregnancy and 19 million have an unmet need for modern contraception. Among these women, this need is greater for adolescents aged 15–19 than for all women of childbearing age, aged 15–49 (64% and 56% respectively). In addition, every year 14 million women give birth in West Africa without receiving the necessary care and 2.4 million opt for illegal abortions, as abortion is only legal in cases of incest, rape or when the pregnancy is dangerous for the mother. It is therefore clear that the lack of care, or of care of sufficient quality, and SRH laws puts women at risk. In some situations, contraceptives are inaccessible due to a lack of financial resources or the unavailability of these products in community health centres or pharmacies.
Furthermore, sexuality in some West African contexts is still taboo, limiting the possibility for girls and women to easily express their needs and enjoy individual freedom in the choices they make. However, in recent years, several community-based associations and projects have emerged that aim to improve the knowledge and ability of girls and women to access their rights, including those related to SRH. Thanks to these initiatives, much progress has been made, but challenges remain, such as reducing unwanted pregnancies, increasing the use of contraceptive methods, providing access to good quality information and recognising the rights of women to take charge of their bodies and make choices in line with their aspirations. This is what the West African Young Feminists Network has been working on since 2018 through several initiatives. Our main mission is to bring the voices of women and girls, especially West African women and girls, into the decision-making processes at the national, sub-regional and international levels, and to uphold our feminist values in order to actively contribute to the improvement of the living conditions of women and girls. To achieve this, we ensure that the commitments that have been made are respected. We are also implementing grassroots actions to involve women and girls in West Africa in determining our priorities and have created a collective feminist movement for equality, collaborating with other members of civil society and communicating our values. For example, Women 7, Women Deliver and the Nairobi Summit are spaces that we have used to defend our interests and propose optimal solutions. We are also present on social media: we have organized a series of Facebook Lives, tweetups and also feminist events in three countries in the subregion with powerful speeches on feminism.
How do you think it would be possible to develop access to better sexual and reproductive health care for girls and women in your country? What are the obstacles encountered in developing such access?
The health system in West Africa, particularly that relating to SRH, is characterized, among other things, by a lack of health infrastructure for adequate care, low investment in the training and care of health personnel and the stigmatization of girls and women by health personnel [153] . In these conditions, medical care for girls and women during pregnancy, after childbirth or following an abortion, during the treatment of an STI or after a major obstetrical complication becomes complex. In order to promote access to better SRH care for girls and women in the region, it is important that all actors in society working in the health sector mobilize together around the single objective of improving SRH for girls and women in order to achieve the Sustainable Development Goals (SDGs) by 2030. This joint action would involve coordination between public entities (governments) and private actors (civil society, including feminist youth groups, NGOs, girls and women) and combining their efforts in a single sub-regional health programme that is clear in terms of objectives, with a greater mobilization of budgetary resources. Beyond the health sector, this collective movement should involve other sectors, such as education, to increase knowledge through awareness-raising and information initiatives, the development for good governance of public policies and funding for the development of human health resources and their equitable distribution within each country. Furthermore, the adoption of universal health insurance in all West African countries could also promote better access to curative and preventive care, including SRH.
While we consider West Africa as a single entity in this reflection, it remains a sub-region composed of several countries, each with its own cultural context. However, these cultural contexts are very similar and play a very important role in health. SRH programmes in in West African countries are often confronted with cultural and societal barriers, such as sexism, rumours about contraception, religion, taboos surrounding sexuality, lack of reproductive choice and access to education. Far from being an obstacle to the implementation of the proposals mentioned, the cultural context represents a challenge; the challenge of adapting programmes to the cultural context and overcoming barriers. Moreover, in some countries, SRH is not a government priority. Our programmes may not therefore receive the attention of policy makers, or the resources needed for their implementation. Other frequent challenges in our mission to promote girls’ and women’s access to SRH care are discrimination and prejudice against activists. In addition, the social norms that require women to begin a family at a given age, i.e. bear and care for children, mean that some women, especially in community settings, show little interest in what we are trying to achieve.
What actions would you prioritize to ensure that more girls and women have access to health care facilities and information to enable them to know their rights, and thus fight against early marriages and pregnancy, female genital mutilation, gender-based violence, etc.?
In West Africa, some populations still find it difficult to discuss sexuality issues and girls and women are still treated as second class citizens despite many initiatives. They are victims of several types of sexist and sexual violence, such as child marriage, female genital mutilation (FGM) and gender-based violence (GBV), which they sometimes consider to be the norm because they are unaware of their rights. To help girls and women be aware of their rights, defend them and claim them, there is an urgent need to improve their knowledge, increase their decision-making power and generally improve their status through social and political changes.
To do this, we suggest:
– technical and financial support for community organizations to distribute information and services through qualified health educators who use engaging methods suited to the realities of the target audience.
– the availability and accessibility of family planning services that enable them to make decisions about their own lives, such as when to marry, when to have children, and how many children to have.
– policies to improve health care, better education and employment opportunities that motivate them to opt for smaller families.
– funding for young feminist associations to continue to advocate for gender equality in all spheres, to develop and run programmes to combat violence against women and girls, gender stereotypes and discriminatory social norms.
These priority actions should promote and women and girl’s decision-making power, the recognition of their rights and the reduction of aggression and violence.
Furthermore, girls and women must be involved in the planning and implementation of programmes and policies for them so that their needs and preferences are truly taken into account. But this will only be possible if governments invest in the potential of civil society actors, especially young feminist associations that work alongside girls and women and work to deconstruct power imbalances. Governments should also make adequate infrastructure available, improve the health care system and address the lack of qualified health personnel in rural areas.
The commitment to gender equality is also reflected in information programmes for both men and women and awareness-raising projects on women’s rights involving men. What types of programmes should be funded?
Involving men in actions for gender equality is an opportunity to prove to men that the cause we are defending is not against them, but rather with them for the emancipation of society as a whole and in particular that of women. The types of programmes to be funded for this purpose would be those organized by feminist movements in which men advocate with women. Making these initiatives known in the sub-region and providing the means for them to communicate their ideas and values could contribute to a change of mentality. Several other programmes also need funding.
These include:
– programmes to deconstruct male stereotypes from an early age and promote a more egalitarian world for future generations.
– education and awareness-raising programmes for boys and men on combating violence against women and girls.
– advocacy to extend and make paternity leave mandatory.
– listening and counselling programmes to support boys and men in their process of changing their behaviour and helping them to integrate the notion of gender equality.
– initiatives to encourage boys and men to commit to a real sharing of domestic responsibilities.
Apart from the types of programmes to be funded, it would be worthwhile considering the development of integrated gender equality policies focusing on women and men rather than separate policies for women and men. This would involve explicitly referring to men and boys in gender equality policies, specifying what their responsibilities may be in achieving gender equality.
What have been the impacts of the Covid-19 health crisis on access to health information and services for young people and women in the region?
According to data provided by governments and health authorities, West Africa has not been seriously affected by the Covid-19 pandemic, but it has not been without consequences.
Regarding access to information, the health measures put in place by governments to protect populations prompted some technical and financial partners to put SRHR projects on hold during the first wave in 2020. As a result, in some regions, awareness-raising, education and knowledge-raising activities on the subject have been suspended. This situation has therefore hampered the dynamic of continuous information to protect vulnerable populations from unwanted pregnancies, sexually transmitted infections, illegal abortions and violence. With the exception of data on the health crisis, there is currently no data to accurately assess the effects of Covid-19 on SRH indicators. It could be said that the coronavirus has stolen the limelight from other pressing public health concerns.
With regard to access to health services, it has been noted in the sub-region that, despite the pandemic, hospitals are still providing services. However, curfews, isolation, social distancing, fear of being infected by the coronavirus, the high cost of medicine and transportation are all factors that limit girl’s and women’s accessibility to health services. The reallocation of resources and priorities in all sectors, including SRH services, to develop a better response to Covid-19 has also had repercussions on access to health services. This can lead to increased maternal mortality and morbidity, as well as higher rates of teenage pregnancy, and unmet needs relating to family planning, HIV and sexually transmitted infections. In addition, data available in the press indicates an increase in domestic violence and a potential increase in unwanted pregnancies due to confinement [154] .
What programmes have been or could be developed at regional level to address this?
In several countries, hotlines have been set up to enable women and girls who are victims of violence to report aggressive behaviour or a violent situation without leaving their homes.
We propose that arrangements be made to ensure that routine health services are maintained during the pandemic period, particularly SRH care through financial support programmes for girls and women to better cope with the economic crisis caused by the pandemic. We also propose programmes to strengthen health care systems to ensure that services other than those mobilized against the pandemic are not disrupted, and that home visiting programmes for groups at particular risk, such as pregnant women, people living with HIV and people with disabilities are not affected.
What concrete commitments do you expect from the Generation Equality Forum, especially concerning the part devoted to the promotion of sexual and reproductive rights?
Given that the aim of the Generation Equality Forum (GEF) is to take stock of progress and develop a programme of concrete measures to achieve gender equality by 2030, we expect in concrete terms that:
– governments commit to making comprehensive sexuality education a reality.
– governments deploy funding at the international level for the implementation of interventions suited to the needs of girls and women over a relatively long period of time.
– governments significantly increase their financial support to civil society organizations, including young feminist organizations, and build on their expertise in SRHR to take meaningful action.
– governments remove the current administrative barriers that make it difficult for feminist organizations to access funding, and that the methods of granting this funding are flexible, accessible, multi-annual, and defined in agreement with feminist organizations, and that they are adapted to the realities, the priorities for action and women’s needs. By doing so, governments will ensure the implementation of women’s organizations’ action plans, the strengthening of their structures and a synergy between actions resulting in greater impact.
– governments guarantee the protection of feminists and give them a place at the discussion table.
What are the best funding channels in this area?
For SRHR projects, there could be partnership agreements, grants, conferences and events at all levels, sponsorships and calls for projects.
It should be made clear that feminist associations currently receive little financial support, particularly on the issue of violence against women and girls. The Generation Equality Forum is therefore an ideal channel and an appropriate occasion for governments to engage with feminist organizations.
Which international bodies do you find most effective in promoting SRHR?
– the annual meeting of the Ouagadougou Partnership
– UNAIDS, specifically on the issue of HIV/AIDS, which is pushing for a human rights-based approach
– The Generation Equality Forum
– The UN Commission on the Status of Women (CSW)
– Women Deliver
Burkina Faso, Wendyam Micheline Kaboré
Wendyam Micheline Kabore is Executive Director of the Initiative Pananetugri pour le Bien-être de la Femme (IPBF) (Pananetugri Women’s Well-Being Initiative). The IPBF aims to promote the development of women and girls in Burkina Faso and in the West African sub-region.
How would you describe the situation in your country regarding women’s access to the right to sexual and reproductive health? Can you tell us about the actions you are carrying out in this field?
In Burkina Faso, the situation of women’s access to sexual and reproductive health and rights (SRHR) has improved significantly in recent years, but several challenges remain. The rights of girls and women to enjoy their bodies and make decisions about them continue to be ignored in this highly patriarchal country. Young girls drop out of school because they become pregnant or are married early. Women often die as a result of insufficient time between pregnancies and backstreet abortions. Faced with this situation, the Burkina Faso government and civil society organizations (CSOs) are making a point of promoting the rights of women and young people regarding sexual reproductive health (SRH). The various parties are working in particular to reduce the rate of abortions, especially backstreet ones, through the implementation of policies and preventive actions. In 2015, the country passed a law allowing abortion, in particular in cases of rape, incest, or if the health of the mother or foetus was at risk. However, action has been slow to follow. This law remains unknown to the general public and is also often unknown within the medical profession or not applied due to personal judgement. The procedures for accessing justice are also very complex and victims are ill-equipped and under-informed regarding legal procedures in this area, resulting in the persistence of practices that are harmful to women, including backstreet abortions often with terrible consequences, such as infertility or even death.
The Pananetugri Women’s Well-Being Initiative (IPBF) cannot remain inactive regarding this situation. Aware that the fight to improve women’s access to SRHR involves synergy between actions, our organization is playing a role in improving the situation through several actions. Our activities include awareness raising and advocacy. We are working on developing awareness of SRHR in groups of leading young women and girls. They are experienced in SRHR issues and are able to raise awareness among their peers.
The establishment of leadership clubs in high schools, colleges, vocational training centres and girls’ associations is an approach favoured by the IPBF. The young girls in charge of running these clubs are trained in leadership and equipped to deal with issues such as gender-based violence (GBV), sexual reproductive health and everyday life skills [155] in order to ensure the smooth running of the clubs, as well as the training of other young girls who are members of these clubs.
In terms of advocacy, emphasis is placed on the SRHR of young people, especially girls. Early, unwanted pregnancies and backstreet abortions are harmful for young girls and put them at a considerable long-term disadvantage.
How do you think it would be possible to develop access to better sexual and reproductive health care for girls and women in your country? What are the obstacles encountered in developing such access?
To develop girls’ and women’s access to better medical care in terms of SRH in Burkina Faso, we focus on three main areas: advocacy, awareness raising and capacity building. The challenges relating to medical monitoring are multi-layered.
We advocate for the state and its partners to take greater account of the specific sexual and reproductive health (SRH) needs of girls and women to invest more in SRH, to implement policies to better address these needs and to improve the quality of care and women’s and girl’s access to SRH services. Reports of studies, surveys and activities reveal the inadequacy of the medical profession in providing an effective service adapted to the SRH needs of girls and women. Personal judgement, reluctance to offer certain services to girls and lack of skills in specific SRH areas are barriers to the use of SRH services by adolescents and young adults. This results in a low rate of medical follow-up in SSR, because young people come for consultation when they are obliged to, but as soon as a solution is found, they do not come back for follow-up.
Awareness raising includes providing accurate information about SRHR, attempting to deconstruct some of the social norms that perpetuate inequalities in access to SRH services, and informing people about good SRH practices for the well-being of the community, especially women and girls. To achieve this, we organize several activities, use various awareness-raising channels and involve all stakeholders.
Finally, we are working on capacity building for youth leaders to support advocacy and awareness raising. Awareness among young people is a great asset, hence the importance of developing the skills, knowledge and abilities of young girls – and boys – enabling them to make informed choices, behave responsibly and generally have a better future.
However, we are facing some difficulties in the implementation of these different actions. These include social and cultural norms, and individual reluctance. Some harmful practices against women are difficult to overcome. They are generated and maintained by the patriarchal system and its corollaries which are vectors of discrimination and of violations of women’s rights in Burkina Faso. This hostile environment is a major obstacle to the respect of girls’ and women’s rights. Some subjects remain taboo, and so result in the perpetuation of gender-based violence.
What actions would you prioritize to ensure that more girls and women have access to health care, facilities and information to enable them to know their rights, and thus fight against early marriages and pregnancy, female genital mutilation, gender-based violence, etc.?
In Burkina Faso, political will has enabled the adoption of policies favourable to SRHR. The Ministry of Health, in collaboration with the ministry’s sectoral departments, has put in place flagship measures, thus maintaining the country’s leadership in this area.
Burkina Faso has made significant efforts at the policy and programmatic levels: a policy of delegation of family planning (FP) tasks, inclusion of FP in the National Economic and Social Development Plan (PNDES), and development of the National FP Acceleration Plan (PNAPF 2017–2020), which is currently under review. It is maintaining this momentum with the recent adoption of the policy of free PF care and services, the revision of the Public Health Code and SRH policies, standards and protocols, and the various policies and initiatives in the fight against cervical cancer – including free screening and treatment of precancerous lesions since 2016, and plans to include the HPV vaccine in the general vaccination programme, etc.
Furthermore, the country is involved in several commitments to SRHR and has actively participated in several regional and international consultation bodies on SRHR: the Ouagadougou Partnership, Family Planning 2020, International Conference on FP, etc.
These dynamic initiatives might lead one to believe that government actions are covering the real needs of the population. Unfortunately, there are still shortcomings at all levels of the intervention chain.
We believe that certain actions are essential and necessary for the respect of the rights of girls and women in Burkina Faso, these include:
– the integration of comprehensive sexuality education (CSE) into the formal and non-formal education system, promoting a wider awareness of SRH and gender-based violence among students and teachers.
– strengthening access to SRH services for adolescents and young adults by training health providers in specific approaches to young populations, in order to increase their capacity to offer targeted services adapted to the needs of young people.
– the creation of spaces dedicated to young people and equipping of these spaces to allow young people to benefit from recreational areas for leisure and educational activities.
– raising of awareness /communication to encourage changes in behaviour. In addition to developing the capacities and skills necessary for young people to take their destinies into their own hands, it is essential to strengthen public communication campaigns, in order to participate in and contribute to the deconstruction of sexist and gender stereotypes and thus foster an environment that respects the rights of girls and women.
– the carrying out of advocacy initiatives. The implementation of a legal system that has all the necessary texts and decrees to protect victims of gender-based violence is crucial.
– the establishment of legal clinics offering assistance to victims in obtaining their rights and compensation for damages.
The commitment to gender equality is also reflected in information programmes for both men and women and awareness-raising projects on women’s rights involving men. What types of programmes should be funded?
In the analysis of the current situation carried out by the IPBF in 2019, an initiative that emerged as being very beneficial for young girls and women was information campaigns for parents, and traditional and religious leaders regarding knowledge and respect of the rights of young girls. These campaigns are essential to change harmful attitudes and underlying social norms that hinder the full development of girls and women. It is necessary to carry out advocacy actions within governmental structures for the voting and/or application of texts favourable to the promotion of the rights of girls and young women.
By translating these two recommendations into action, we can articulate specific programmes, both for adolescents and young adults, and for the general population, including men and women, to achieve gender equality goals. On this basis, funding should be targeted more towards specific programmes for young people, designed by young people and implemented by them. The involvement of young people is essential, especially young girls, who are best placed to talk about their difficulties and express their specific needs. The issue of resource mobilization is central to our work, hence the IPBF’s establishment of the Pananetugri Fund, which was the first recommendation of the 2019 study. In response to the increased resource mobilization challenges within organizations led by and made up of girls and young women, we confirm that the funding of initiatives developed and implemented by young women is essential.
Gender-sensitive and inclusive programmes need to be promoted and supported, because today it is very important to focus on “gender mainstreaming” – the integration of gender considerations into new policies and actions. The funding of programmes that integrate approaches that include women and men, taking into account their specificities, is to be encouraged. Men and women’s attitudes need to be developed, through an emphasis on awareness-raising programmes for the whole population, and specific advocacy targeting all social categories. Programmes that address social and cultural constraints, that contribute to the deconstruction of sexist and gender stereotypes and bring about significant change in the current situation are complementary and necessary.
Finally, programmes to improve the legal environment in Burkina Faso should be funded by supporting the adoption of legal texts favourable to the rights of girls and women and by training actors in the justice system with a view to optimizing their work.
Schools also have a role to play in combating gender-based discrimination, sexual orientation, etc. and in promoting comprehensive sexuality education. What programmes are or could be developed in this direction in your country and, if they exist, are there any collaborations at the regional level?
Education in Burkina Faso is at a crossroads, after several experiments and reforms affecting both form and content. Education in Burkina Faso continues to be restructured, with recent reforms that are a source of controversy.
It is also affected by natural disasters, such as floods, and the security crisis from which the country has suffered in recent years. Data collected from the technical secretariat for education in emergencies indicate that, as of 5 February 2021, 2,212 schools are closed. These school closures directly affect 316,040 students (168,463 boys and 147,577 girls), and 12,366 teachers (7,889 men and 4,481 women).
This alarming situation has led to several initiatives to reintegrate pupils into the school system. Several actors are involved, primarily the ministry, development partners, and organizations working on education issues. Girls’ and women’s rights organizations, including the IPBF, are also addressing the issue by creating specific projects. For example, the Accelerated Education Strategy, adopted in 2006 by the Ministry of Education and the IPBF, on behalf of civil society organizations, implements a data-driven advocacy project for girls’ education in crisis situations in Africa. There are many other initiatives, but few of them integrate the issue of rights, the fight against gender-based discrimination, or the issue of comprehensive sexuality education. This last point has met with opposition in Burkina Faso. Last April, a statement by the Minister of Education left those advocating for the introduction of comprehensive sexuality education speechless. In an interview, the Minister declared: "There is the issue of sexuality in schools, which is an increasingly serious phenomenon, especially with the attempts by some technical and financial partners to get us to accept comprehensive sexuality education. The word “comprehensive” implies an acceptance of homosexuality [156] .”
In view of the interventions on this subject, we believe that there is an urgent need for a specific communication through a programme to provide the necessary clarification on the introduction of CSE into our school system. As civil society organizations, we follow the recommendations of beneficiaries and other project actors to contextualize the different themes, concepts and strategies related to the topic.
Responses should be appropriate to the context, and above all the language used by actors should be understandable to the majority of people.
Awareness-raising and advocacy programmes for the « introduction of family life education » (a formulation adopted by Burkina Faso to replace « comprehensive sexuality education ») should be encouraged and implemented as soon as possible, in order to protect the health and improve the futures of young girls and boys.
There is therefore a need to develop gender-sensitive education policies, to revise teacher training curricula to include family life education, and to include subjects that can teach values of equality and equity in the school environment. Textbooks that perpetuate sexist stereotypes, discrimination and gender inequality should be removed from the education programme. To achieve this, teacher training needs to be reformed.
What concrete commitments do you expect from the Generation Equality Forum, especially concerning the part devoted to the promotion of sexual and reproductive rights? What are the best funding channels in this area? Which international bodies do you find most effective in promoting SRHR?
Since the World Conference on Women (Beijing, 1995), there has been no major global action on SRH by governments or civil society. Fearing a decline in these rights, France, Mexico and UN Women decided to celebrate the twenty-fifth anniversary of that milestone through the Generation Equality Forum (GEF) initially planned for July 2020 but postponed due to the Covid-19 crisis. This international event will be held in Paris from 30 June to 2 July 2021 and will bring together, mainly by video conference, not only actors from civil society and feminist movements, but also governments, researchers, foundations and companies. As such, the upcoming forum is a high point for the commitment of gender equality advocates from all fields. This global consultation framework of advocates for girls’ and women’s rights is an opportunity to take concrete action and achieve immediate and lasting change for girls and women. Through the establishment of the six coalitions for action, the issues of girls’ and women’s rights will be addressed in their entirety.Nous attendons du Forum génération égalité des recommandations à l’endroit des différentes parties (États, organisations non étatiques, partenaires techniques et financiers, société civile…) pour une meilleure protection des droits à la santé sexuelle et reproductive. Cela inciterait les États à adopter des mesures fortes et concrètes, qui permettraient de réduire les inégalités de genre dans l’accès aux services de santé sexuelle et reproductive et de mieux lutter contre les pratiques néfastes pour les filles et femmes, comme les avortements clandestins, les mutilations génitales féminines.
We expect the Generation Equality Forum to make recommendations to the various parties (governments, NGOs, technical and financial partners, civil society, etc.) for better protection of SRHR. This should encourage governments to adopt strong, concrete measures to reduce gender inequalities in access to SRH services and to better combat practices that are harmful to girls and women, such as backstreet abortions and female genital mutilation (FGM).
These commitments, which will be made primarily by state actors, development partners and other stakeholders, should be translated into action, and given form in clearly defined programmes to address the challenges girls and women face in their daily quest for access to sexual and reproductive rights.
In Africa, and mainly in in the West, a region suffering from a variety of problems – natural disasters, the health crisis and the security crisis – the challenges are enormous. Unfortunately, the importance of unmet needs in relation to vulnerability of the population raises the question of the prioritization of national issues. Development partners, the United Nations system, and diplomatic representations are, currently, the main providers of resources in Burkina Faso.
Several projects are being developed by major world powers, but they are focused on security issues, unfortunately leaving development issues as the responsibility of the Burkina Faso government, which is struggling to address them effectively. For civil society actors, international NGOs are the most targeted in the mobilization of resources. The World Bank, the World Health organization (WHO), the United Nations Population Fund (UNFPA), international NGOs working on the issue, African regional institutions and the African Union (AU) are all structures, organizations and bodies capable of carrying the fight for access to SRHR services for everyone in Burkina Faso and in the sub-region.
Oumou Salif Touré is a member of the Young Feminists Network of West Africa which brings together activists and feminist activists from French-speaking West Africa who present the views of girls and women to decision-making bodies at local, regional, national and international levels.
How would you describe the situation in your country regarding women’s access to the right to sexual and reproductive health? Can you tell us about the actions you are carrying out in this field?
Mali has relatively weak sexual and reproductive health (SRH) indicators, particularly in terms of the promotion of sexual and reproductive rights (SRHR) for young people and adolescents and even more so for women. Access rates to family planning and contraceptive methods are low overall, and rates of early pregnancy and marriage and gender-based violence are high, with strong regional disparities.
In the latest United Nations Development Programme (UNDP) census published in 2019, Mali was ranked 184 (out of 189) in the Human Development Index (HDI). In addition, there has been great insecurity since 2012 due to jihadist attacks and intra-community conflict. This reflects deep economic, health and social inequalities that undermine the country’s growth and the well-being of the population.
Although the environment is hostile, targeted action is being taken on these issues, with a relatively strong, though largely unenforced legal framework, an active civil society and a wide range of actors.
Cultural sensitivities and taboos surrounding sexuality often prevent citizens from learning about sexual and reproductive health and care, making it difficult for governments to address these issues.
How do you think it would be possible to develop access to better sexual and reproductive health care for girls and women in your country? What are the obstacles encountered in developing such access?
Despite this hostile climate, characterized by the government’s inability to pass the bill for comprehensive sex education, the Machiavellian approach of certain religious leaders who are mortgaging the future of an entire generation, and the inaction of a large proportion of these young people, some young people are nevertheless on the ground during the day in IDP camps, in schools, railway stations, on the radio and TV, in the evenings with families, meeting friends for tea, all are occasions for informing people, raising awareness and providing guidance on sexual and reproductive health issues.
Some of the barriers arise from age restrictions that require parental or decision-maker consent for minors, while others arise from social norms whose main effect is to inhibit young women’s ability to obtain information about sexuality and reproductive health issues. These barriers discourage adolescents from seeking medical help or information at a time when they are beginning to be sexually active and need such information for their own safety. Child marriage and early pregnancy have serious negative implications for girls’ ability to enjoy their right to education and health.
The requirement of third-party consent is another significant problem. Adolescents often face the challenge of being able to access sexual and reproductive health information and services only with the consent of a parent, guardian, spouse or doctor. Women’s access to health services or to clinics that provide these services is hindered on the grounds that the woman does not have the permission of her husband, partner, parents or health authorities, because she is single or simply because she is a woman, which is contrary to law no. 02–044 on sexual and reproductive health in Mali.
To ensure that women and girls are welcomed and that their needs are taken into account, there is a need to develop advocacy for the creation of a specific budget line for the purchase of contraceptive products, since the high prices at which they are offered by public health services is a deterrent. There is also a need to communicate tirelessly about the existence of the SRH law in Mali, as most actors working in this field seem to be unaware of it. This lack of knowledge results in the violation of the rights of the beneficiaries in full public view.
The numerous human rights defenders, civil society organizations and health professionals working on behalf of women’s sexual and reproductive health and rights in Mali are also affected by this problem. In some contexts, violence, threats, hate speech and smear campaigns, including by religious leaders, continue to target both human rights defenders advocating for gender equality and women’s sexual and reproductive health and rights and health professionals who provide care in this area.
All too often, hostile reception by providers in health centres, age discrimination, judgement of the service recipient’s choices or outright refusal to provide a contraceptive method drive women and girls in need away from public hospitals. By going there, they also risk encountering people they know. The discretion that they were seeking in adopting a contraceptive method then completely disappears. For this reason, it is important to emphasize the need to create and run specialized sexual and reproductive health centres with trained providers to for women in need.
While each individual working in a health facility is entitled to his or her own values regarding the sexual behaviour of young people and adolescents, it is imperative that providers recognize that adolescents and young people, like adults, have basic sexual and reproductive health rights, including the right to be treated with dignity and respect, the right to access a range of services, including contraception, that are accessible and affordable, and the right to private and confidential services. These rights require providers to balance their personal values with their professional duty to provide appropriate sexual and reproductive health services to young people and adolescents.
What actions would you prioritize to ensure that more girls and women have access to health care, facilities and information to enable them to know their rights, and thus fight against early marriages and pregnancy, female genital mutilation, gender-based violence, etc.?
In terms of priority, communication to change generational behaviour is needed. It is not the classic process of communicating and raising awareness for behaviour change, but rather the process of protecting the new generation. Common ground will not be found in a patriarchal and conservative society like Mali.
It is important that programmes are implemented throughout the community, not just for young women and men. Building strong, coherent support systems around young people can take many forms. Adolescents and young people are not a homogeneous group, needs may vary according to age, marital status or livelihood, etc.
It is important to direct awareness raising at younger targets but also future citizens: parents that have already been victims of this obscurantist system that consists of keeping them bound to harmful traditional practices under the guise of religion or by accusing the few human rights defenders of « taking money from the white man ». A new generation is emerging that needs help and wants to be different. It is to them that awareness-raising projects must be addressed, it is to them that the messages for behavioural change must be addressed, they must be made to understand the importance of studying, of becoming responsible, independent, of fulfilling their duties, of knowing and claiming their rights. This is how the future generation will be protected and stand up to the evils that plague our society (gender-based violence, child marriage, early pregnancy, etc.).
The use of social media as awareness-raising channels opens up new possibilities for accessing information. Girls and women can learn about their bodies in a more easy-going, relaxed environment, and about the different modern methods of contraception; they can also learn simple measures that can save the lives of children, girls and women. There are many existing examples of how, for example, the dissemination of testimonies of victims of gender-based violence (GBV) who have been able to rebuild their lives has been a powerful means of educating other women, and encouraging them to speak out against violence. The fact that women with little or no education are shown to be role models or influential leaders who participate in decision-making proves that women and girls are able to gain confidence and discuss decisions with their partners and families on issues such as health, girls’ education, fighting against child marriage and campaigning for women’s work.
The commitment to gender equality is also reflected in information programmes for both men and women and awareness-raising projects on women’s rights involving men. What types of programmes should be funded?
We are all responsible for a more feminist vision. Equality between women and men is a requirement of democracy, the struggle for equality is a universal struggle. Everyone must be involved: the government, local authorities, elected representatives, parents, youth services, associations, etc.
It is not about cancelling the biological difference between men and women, but about working towards more equality and fighting against sexist and sexual violence.
And it is not just a “women’s issue”, it is a social justice issue, hence the need to involve men in the projects and programmes implemented. Obtaining commitment from men can be a useful approach in this struggle. Positive masculinity must be at the heart of actions, men and boys are seen as partners and agents of change to actively promote gender equality and transform inequitable or harmful gender norms, including harmful forms of masculinity. Ultimately, this approach aims to improve outcomes so that men and women can live in harmony while respecting women’s free will.
We need to insist on free will, because there is sometimes a tendency to believe that without men, projects for equality, sexual and reproductive rights are doomed to failure. This would perpetuate the patriarchal system. Our lives are not forever tied to this system. Women and girls are more than a powerful minority, who can assert themselves by raising “he for she” boys, and thereby forging the character of future men. Stereotypes will be deconstructed and an egalitarian society will emerge, with or without the help of men.
What have been the impacts of the Covid-19 health crisis on access to health information and services for young people and women in the region? What programmes have been or could be developed at regional level to address this?
Comprehensive sex education in Mali is a real headache! Despite the efforts of civil society, the plan to include comprehensive sex education has been brushed aside by religious leaders and their followers under the pretext that we want to teach children to be “homosexuals”! Following a large media protest movement on social media accompanied by meetings and marches in the capital’s public squares, the project remained in the embryonic stage.
Adolescents should be provided with medically accurate, comprehensive and appropriate sexual and reproductive health information and education adapted to their level. It has been found that comprehensive sexuality education can increase behaviours conducive to protecting sexual health.
Access to information is crucial to raising awareness about sexual and reproductive health and rights among adolescent girls and boys. In Mali, biology lessons on reproduction are not enough, nor are courses on family life education. There is little information on gender-based violence, rape or family planning. Young people’s knowledge is often superficial and incomplete, and influenced by the teacher’s own beliefs or misconceptions. The truthfulness of the facts depends on their mood, beliefs and sometimes their political orientation.
Sex education in schools becomes a necessity when parents have given up. It is up to the school to take over and break the taboos associated with sexuality, in a manner appropriate to the age of the child or adolescent.
In order to support a new generation of young people capable of making informed choices, they must first be provided with objective information about their sexuality. Adolescents need to be listened to as part of this comprehensive sexuality education. They are not just recipients of programmes; they are the primary actors. They need to be in possession of up-to-date and relevant information to become allies later on. The government needs to understand that investing in comprehensive sexuality education ensures better quality education for these young people, especially young women and girls. If more girls stay in school and are equipped with the knowledge to make critical decisions, the impact will be invaluable.
Beyond the technical and biological aspects of conception and motherhood, it is important to address issues of sexual and reproductive rights of young people, the relationship between boys and girls, gender inequalities and stereotypes that dictate the society model and gender roles. However, the competence of facilitators, teachers and health workers and their knowledge of SRHR need to be ensured, and the inclusion of comprehensive sexuality education in school programmes should be put back on the table.
What concrete commitments do you expect from the Generation Equality Forum, especially concerning the part devoted to the promotion of sexual and reproductive rights? What are the best funding channels in this area? Which international bodies do you find most effective in promoting SRHR?
The politicization of sexual and reproductive rights issues contributes to their neglect by donors, even though girls’ and women’s health is seen as a condition for the achievement of the Sustainable Development Goals (SDGs) and the acceleration of economic growth that can result from a rapid decline in a country’s fertility and subsequent change in the age structure of the population.
In developing countries, unmet needs are considerable, and funding is insufficient. The Covid-19 pandemic has contributed to these difficulties.
The re-adoption of the Mexico City Policy [157] (“Global Gag Rule”) by the United States in 2017 has a disastrous impact on the level of international funding available for SRHR. Many young people have been deprived of information and contraceptive methods, and many information centres dedicated to sexual and reproductive health have been closed.
France’s leadership on the SRHR Action Coalition represents a major opportunity to strengthen political commitments to the achievement of SRHR and to ensure that these commitments are translated into sufficiently ambitious funding to help fill the funding gap at the international level.
Nafissa Hassan Alfari is president of the Nigerian Cell of Young Female Leaders (CNJFL). The CNJFL works to promote the education of girls and women, leadership and female entrepreneurship.
How would you describe the situation in your country regarding women’s access to the right and to sexual and reproductive health? Can you tell us about the actions you are carrying out in this field?
In the Niger, the issue of women’s access to sexual and reproductive health rights is evolving. Progress is being made because today women and girls are asserting their sexual and reproductive health rights (SRHR). Taboos surrounding certain issues, such as managing menstruation, are being lifted. We have a contraceptive prevalence rate of over 20% and our ambition is to see it double. Women are increasingly using contraceptive methods and have access to health services and contraceptive methods in urban areas. Communities are beginning to realise the importance of talking about sexual and reproductive health (SRH), and also the fact that that access to sexual and reproductive health is a basic right for women. We also have a law on reproductive health, that dates from 24 May 2006. But despite all these advances, women and girls do not have full access to all their sexual and reproductive health rights. For example, women cannot access family planning without their husband’s approval. Husbands frequently come to the health centre with their wives to choose the contraceptive method and impose their opinions. Due to a still current misinterpretation, women who use contraception are likely to be judged by society as wanting to stop having children or as not wanting to be mothers, whereas family planning simply means determining when births occur, so they can be spaced out. Women’s right to pleasure is not fully recognized because genital mutilation is still practised, although it is becoming less frequent. This is a very important issue, because in the Niger a woman without children is stigmatized by society, since it is considered normal for women to have many children. As part of women’s access to sexual and reproductive health and rights, we carry out awareness-raising activities on menstrual hygiene management and on women’s reproductive development and functioning, we have also set up circles of influence where women and girls meet to discuss these issues with a health specialist who provides them with the necessary information on sexual and reproductive health. We also sit on the national coalition of youth ambassadors on sexual and reproductive health and work with other structures, such as Lafia Matassa, to raise awareness of sexual and reproductive health among young people and women.
How do you think it would be possible to develop access to better sexual and reproductive health care for girls and women in your country? What are the obstacles encountered in developing such access?
To promote access to-sexual and reproductive health care for girls and women in Niger, women must be made to understand that they have SRH rights, that they have the possibility of benefiting from these rights and, to achieve this, they must be made aware of sexual and reproductive health. Conditions should be improved so that they have access to better medial services in this area. And this necessarily involves the creation of health centres that deal with sexual and reproductive health issues and specifically respond the needs of women in the most remote villages. All women, wherever they are, should have access to these services, so that they can be given appropriate care. The long distance they currently have to travel to be treated at health centres prevent them from returning regularly; they often do not return for a year or two after their first appointment. The medical staff must be trained to treat women confidentially, without judgement, and, most importantly they must be able to recognize their problems, and put them at ease when they come to the centres in order to meet their sexual and reproductive health needs.
Husbands, men, boys, religious and traditional leaders must be involved in implementing projects and programmes to promote women’s access to sexual and reproductive health, so that they too be a part of recognizing the importance of women’s sexual and reproductive health rights, with a view to the whole community adopting a more favourable attitude to the sexual and reproductive health rights of women and girls. Such involvement enables women to go freely to health services without fear of judgement and to benefit from this fundamental right without any obstructions. The first and biggest obstacle for projects and programmes addressing women’s and girls’ access to sexual and reproductive health in their communities is the misinterpretation of the term “sexual and reproductive health”. Because when we talk about sexual and reproductive health, communities imagine that it is about preventing women from becoming pregnant or giving birth, or other prejudices fuelled by the patriarchal system. At the same time, there is also the fact that women and girls lack information on sexual and reproductive health because they live in too far away from health centres. Finally, it should be noted that young girls are generally stigmatized in health centres because of their marital status.
What actions would you prioritize to ensure that more girls and women have access to health care, facilities and information to enable them to know their rights, and thus fight against early marriages and pregnancy, female genital mutilation, gender-based violence, etc.?
To ensure that more girls and women have access to health care facilities and information to enable them to know their rights, to fight against early marriage and pregnancy, female genital and gender-based violence, actions focus primarily on the legal framework. There is an urgent need to introduce a specific law to fight against gender-based violence and ensure that people are aware of it, and that it is effectively applied. Beyond the legislative framework, there is also a need to implement policies and programmes to ensure that communities take into account the women’s right to sexual and reproductive health. This would enable an awakening of the collective conscience: women must be considered as independent human beings with rights; this is a necessary condition for their emancipation and development in society. There is also a need to focus on female leadership by educating girls from an early age to be aware of their potential and of their rights and to demand that these rights are respected. In Niger, there is a decree on the protection, support and accompaniment of girls in their schooling, the government has thus made a commitment to promoting the education of young girls. Unfortunately, the implementation of this decree is not effective. This is why it is important to mobilize and involve all stakeholders working in the field of education to support the Niger government in its struggle to promote girls’ education.
It is also crucial to increase advocacy in the fight against child marriage and early pregnancy among actors working in the field, community and religious leaders, because they are the gateway to reaching communities. Advocacy actions must also concern the Niger authorities, and national elected representatives because they are the ones who propose and vote on the laws. It would also be preferable, for greater impact, if these advocacy actions were carried out by the girls themselves, because they are the ones who can most legitimately pursue such actions. Women need to be empowered by being involved in decision-making bodies so that they communicate women’s concerns relating to sexual and reproductive health. It is also necessary to set up toll-free numbers that they can call and easily get information on sexual and reproductive health and on gender-based violence. Finally, community dialogue that addresses women’s rights and gender-based violence should be prioritized.
The commitment to gender equality is also reflected in information programmes for both men and women and awareness-raising projects on women’s rights involving men. What types of programmes should be funded?
The commitment to gender equality is also reflected in information programmes for both men and women and awareness-raising projects on women’s rights involving men. To this end, the types of programmes that need to be funded include projects that take gender into account and that involve community and religious leaders, who are listened to in communities. It is easier to approach a community and to introduce change when its leaders are part of the change process. Awareness-raising programmes that particularly focus on young boys to bring about behavioural change should be taken into account, because everything starts with young people and education.
Schools also have a role to play in combating gender-based discrimination, sexual orientation, etc. and in promoting comprehensive sexuality education. What programmes are or could be developed in this direction in your country and, if they exist, are there any collaborations at the regional level?
Currently in Niger, adolescent and youth reproductive health education is taught in schools, it is included in the SVT (life and earth sciences) and home economics curriculum. Initially, there was a push for a comprehensive sexual health education course, but this was opposed by communities. As a result, the authorities have involved religious leaders in the project’s approach, and have managed to contextualize the subject so as not to offend anyone’s sensibilities. It should therefore be possible to carry out these initiatives at the regional level so that each country can integrate such courses into their teaching programmes. It is also important to target students and schools in anti-discrimination awareness programmes and projects, with an emphasis on living together harmoniously and the importance of accepting differences to include everyone.
What concrete commitments do you expect from the Generation Equality Forum, especially concerning the part devoted to the promotion of sexual and reproductive rights? What are the best funding channels in this area? Which international bodies do you find most effective in promoting SRHR?
We expect the Generation Equality Forum to be an opportunity to strengthen the of all actors involved in the field, it should also be an opportunity to mobilize funding to implement projects and initiatives in a decentralized manner, i.e. focusing on actions as close as possible to the communities concerned. We hope that this forum will enable the government of Niger to mobilize enough donors to scale up the good practices that we have developed in the Niger. The best funding channels for sexual and reproductive health are at the local level, i.e. civil society organizations at the local level, especially youth and women-led organizations. Among the international bodies that are most effective in promoting sexual and reproductive health rights, there is the Ouagadougou Partnership on SRHR, civil society involvement in family planning, the International Conference on Family Planning, and the UNESCO High Level Committee in favour of Comprehensive Sexuality Education in West and Central Africa.
République démocratique du Congo, Jean-Claude Mulunda
Jean-Claude Mulunda is IPAS Director for the Democratic Republic of Congo. IPAS is an international non-governmental organization working globally to increase access to abortion and contraception.
How would you describe the situation in your country regarding women’s access to the right to sexual and reproductive health? Can you tell us about the actions you are carrying out in this field?
The situation regarding access to sexual and reproductive health rights (SRHR) in the Democratic Republic of Congo (DRC) remains complex and confusing. The laws on SRHR, including those on contraception, safe abortion, and the prevention and management of sexual and gender-based violence, contradict rather than complement each other. At the same time, the country is facing a war in its eastern part (North and South Kivu) which is never ending, and which has even spread to the centre of the country (Kamuina Nsapu rebellion in Kasai). Furthermore, one of the strategies used by the armed group is sexual, gender-based violence. A few years ago, the DRC was even described as the « rape capital of the world ». The health system is very fragile, with very little budget allocation at the national level, and is therefore largely dependent on external inputs, which are also subject to diplomatic, security or health restrictions (as evidenced by the Covid-19 crisis and repeated epidemics, including Ebola).
The public health context
The situation of maternal health remains worrying in view of the maternal mortality rates (693 women per 100,000 live births [158] ). This situation is partly the result of the high prevalence of high-risk pregnancies due to the low use of family planning services (7.8% of women in union use modern contraceptive methods [159] ). Sexual and gender-based violence, incest, early and forced marriage, poor access to good quality information, especially for young people, a low level of recognition of SRHR, which do not guarantee choice for women and girls, customs and attitudes, religion, reduced decision-making power for women, including over their own bodies and health, are all obstacles to full access to SRHR. Despite the trend towards improvement, with 18% contraceptive prevalence [160] , unmet family planning and contraception requirements remain high. This explains the need for more women to have an abortion. The lack of safe care unfortunately leads all these women to resort to unsafe care, and unsafe abortions, with all the immediate and subsequent consequences that one can imagine on the well-being of the woman, her life and her rights. Unsafe backstreet abortion is the second highest cause of maternal death in the country. A 2016 study by the Kinshasa School of Public Health in collaboration with the Guttmacher Institute on the incidence of induced abortion in Kinshasa [161] showed that two out of five pregnancies ended in abortion in the Congolese capital with an average of 146,700 abortions per year, or 400 abortions per day or 17 per hour. The same source indicates that the percentage of unwanted pregnancies that end in abortion is estimated at 43% and that almost two-thirds of these women who had an unsafe abortion suffered moderate to severe complications.
The legal context
The Congolese Penal Code criminalises contraception (articles 165 and 166) and abortion (article 178): any promotion of contraception, advertising, sale of contraceptive products or offering of services in hospitals or in the community is prohibited. Access to safe abortion is not allowed either, not even in cases of life-threatening risks to the health or life of the mother and/or the foetus. Rape is considered to be an offence against public decency rather than a serious crime. No rights are recognized for woman, not even the right to have access to good quality information in order to make informed choices.
Furthermore, the Code of Medical Ethics does not recognize the right of women and girls to safe abortions. Unlike the Penal Code, the Code of Medical Ethics recognizes the right of women to access a safe abortion in cases of risk to the mother’s physical health or in cases of foetal malformation incompatible with life. But even in these cases, prior assessment by three different doctors and authorization by an official registrar is required. This makes the process long and often does not allow women to benefit from this exception. Some women obtain the various documents required after the termination period has already passed. They often resort to illegal, unsafe care.
The new public health act published in 2018, a few months after the Maputo Protocol was published in the Official Gazette , making the latter an immediately applicable law, did not incorporate the protocol’s indications, set out in its article 14. The public health act has taken up the controversial restrictions of the Penal Code on access to abortion and leaves women with no choice other than contraception.
The Maputo Protocol, or the “Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa", has been, since its ratification by the country, a unique opportunity for Congolese women and girls to have access to their SRHR, including the possibility to have access to safe abortion. Unfortunately, it took almost ten years before the protocol was implemented. According to Congolese law, the Maputo Protocol first had to be published in the Official Gazette . Hence the advocacy undertaken by international and national organizations between 2008 (year of ratification) and 2018 (year of publication in the Official Gazette ) to obtain its publication, which marked the supremacy of this law over the DRC’s internal laws in accordance with the Democratic Republic of Congo’s Constitution (article 215). The Maputo Protocol has the merit of widening women’s choices by allowing safe abortion in cases of rape, incest, or mental or physical health problems of the mother and or foetal malformation incompatible with life. As mentioned earlier, the Maputo Protocol applied immediately after its publication in the Official Gazette , giving it precedence over local laws.
In practice: Application of the laws
At the judicial level, the application of laws, including the Penal Code, the Code of Medical Ethics, the Public Health Act and the Maputo Protocol depends on:
– the judge’s level of knowledge, in particular of the Penal Code and the Code of Medical Ethics, which, by virtue of their age, are the best known and most enforced, thereby condemning by default women, girls and clinical providers, as well as community health workers involved in seeking care (clients), in orientation (community workers) and in providing safe abortion care as part of the implementation of the Maputo Protocol in the country.
– reluctance regarding abortion. Indeed, some judges, aware of the existence of the Maputo Protocol, prefer to ignore it and pronounce their judgement by referring only to restrictive laws, such as the Penal Code, the Code of Medical Ethics and the Public Health Act. This is due to social constraints and stigma against SRHR, including safe abortion.
– poor knowledge of the new legal texts by the lawyers who are supposed to defend their clients.
At the health system level, as a result of advocacy by national and international organizations for the implementation of the Maputo Protocol, the Ministry of Health has developed and approved comprehensive abortion care standards and guidelines, constituting an important step towards access to safe abortion as outlined in the Maputo Protocol. The standards and guidelines, which are as progressive as possible in their content, offering women more choice and power, indicate who, when, where and how safe abortion care can be offered in the DRC.
While these standards are ready to be used to address the abortion needs of women and girls, there are a few prerequisites to consider, constituting issues requiring action, that we are working on with the various stakeholders, namely:
– the dissemination of these standards and guidelines within the health system, that affect both managers and clinical providers of care in the public and private sectors. This step is important because it allows available clinical providers to offer safe abortion care using methods and technologies recognized by the World Health Organisation (WHO). This also reduces the use of methods that have been declared obsolete, such as curettage.
– training of clinical providers in the new standards, which requires the prior development of training tools. Providers have so far been trained to provide post-abortion care, i.e. management of complications after unsafe abortion, using outdated methods. Hence the need to train them in the use of new methods including medical abortion.
– the availability of abortion facilities is also a big challenge in terms of access to care in the country, not only abortion, but all other basic health care.
– combating stigma within health training, particularly for young people and people living with disabilities who, according to social norms, should not be sexually active.
At the community level, the most important issues are acceptance of the act of abortion, recognition of a woman’s rights to seek abortion when she wishes, and community referral for a reasonable standard of care and psychosocial support for clients and clinical providers [162] . Several ongoing actions need to be strengthened:
– provision of widespread access to the Maputo Protocol
– clarification of values and changing of attitudes towards abortion-, especially for community leaders
– communication to encourage the evolution of social norms
– the promotion of women’s rights and SRHR
– dialogue on SRHR that includes religious representatives
– intergenerational dialogue involving young people to take their needs into account.
How do you think it would be possible to develop access to better sexual and reproductive health care for girls and women in your country? What are the obstacles encountered in developing such access?
Beyond the law restricting women and girls’ access to SRHR in the country, there are other obstacles. Firstly, the low awareness of women and girls of their rights, particularly those relating to health and SRHR. This is because everything concerning sex and reproduction is taboo. Young girls do not have access to information about the various transformations their bodies undergo and what this exposes them to, including possible attacks from sexual predators, nor are they informed about their periods and how to manage them.
Secondly, customs do not promote women’s rights in general, and SRHR in particular. This explains the increase in cases of sexual and gender-based violence, forced and early marriages, and incest.
The influence of religion and religious people on social and political life should also be noted. The conservative religious system has maintained and increased its influence on politicians and other community leaders, which delays the implementation of policies that promote SRHR.
Finally, weak community commitment to women’s rights in general, and to SRHR in particular, deprives women and girls who are victims of abuse (forced marriages, rape, backstreet abortions, etc.) of the social support that is the key to their reintegration into the community and to their empowerment.
What actions would you prioritize to ensure that more girls and women have access to health care facilities and information to enable them to know their rights, and thus fight against early marriages and pregnancy, female genital mutilation, gender-based violence, etc.?
The priority actions in the DRC should, in my opinion, be:
– the implementation of advocacy strategies for the improvement of the legal framework, including the application of international covenants and protocols, such as the Maputo Protocol, the Committee on the Elimination of Discrimination against Women (CEDAW), as well as their harmonization with local laws through the updating of the latter.
– strengthening national ownership of the process of promoting and protecting women’s rights and SRHR through the involvement of community and religious leaders, whose capacities must first be strengthened, and their values clarified.
– strengthening community cohesion around SRHR through the establishment of dialogue between leaders and communities and intergenerational dialogue. This would make it possible to highlight recent developments (in values, technologies, etc.) and to adapt laws and social considerations.
– the development of communication and awareness-raising strategies aimed at women and girls so that they can know, claim and benefit from their rights.
– women’s empowerment through the promotion of self-managed abortion and contraceptive care, accountability of the health system and the community.
– the integration of SRHR into all gender promotion programmes.
The commitment to gender equality is also reflected in information programmes for both men and women and awareness-raising projects on women’s rights involving men. What types of programmes should be funded?
Programmes that encourage men’s participation, including those related to positive masculinity and gender promotion, should be funded. The violence and lack of empathy displayed by men are the result of toxic masculinity. These stereotypes are a legacy passed from generation to generation that ignores or is unaware of its negative consequences on the well-being of women, their autonomy and their contribution to the country’s development. Integrated programmes should be favoured, that address SRHR as a whole as part of human rights, with no one being excluded.
Schools also have a role to play in combating gender-based discrimination, sexual orientation, etc. and in promoting comprehensive sexuality education. What programmes are or could be developed in this direction in your country and, if they exist, are there any collaborations at the regional level?
Schools plays an important role in the sexuality education of young people. In the DRC, there is a case for updating the life education course to include gender, comprehensive sexuality education and SRHR in general. The current life education course reinforces toxic masculinity and does not give young people a full range of information. It does not offer choice or autonomy, but rather creates a gap between what young people learn at school and the reality they experience in their daily lives.
What concrete commitments do you expect from the Generation Equality Forum, especially concerning the part devoted to the promotion of sexual and reproductive rights? What are the best funding channels in this area? Which international bodies do you find most effective in promoting SRHR?
The situation in sub-Saharan Africa in general, and the DRC in particular, shows that international legal instruments are needed to promote SRHR in the southern countries. In this case, national laws need to be harmonized to bring them into line with the country’s international commitments. This requires advocacy at the highest level through diplomatic missions, development aid, and bilateral and multilateral cooperation. In terms of funding channels, it is preferable to increase funding to local organizations for which international organizations provide technical support and assistance building their capacities. There is therefore a need to ease funding conditions for local organizations, particularly feminist organizations and coalitions that advocate for SRHR, to encourage projects that strengthen national ownership through community participation, and finally to promote programmes that integrate SRHR.
Fatou Ndiaye Turpin is a family planning champion and executive director of the Réseau Siggil Jigéen (RSJ) (Siggil Jigéen Network). The Siggil Jigéen Network is an NGO committed to the improvement of the status of women and the promotion and protection of women’s rights in Senegal.
How would you describe the situation in your country regarding women’s access to the right to sexual and reproductive health? Can you tell us about the actions you are carrying out in this field?
Despite concerted efforts by the government, NGOs and the international community, the maternal mortality rate remains too high in Senegal, with more than 236 women per 100,000 live births according to estimates by the UN system in 2017 [163] . The high maternal mortality rate can be attributed not only to the inadequacy of the health care infrastructure, but also to social and cultural forces that deny women the right to health throughout their life cycle. Early marriage and pregnancies, female genital mutilation/cutting (FGM/C) and the fact that motherhood is considered a woman’s duty are factors contributing to a high maternal mortality rate. The government of Senegal must take all necessary steps to guarantee women’s rights to safe motherhood.
Induced abortion is illegal and punishable by imprisonment and a fine. Therapeutic abortion is allowed under the Code of Medical Ethics but is not explicitly recognized by the Penal Code. Senegal has retained these repressive laws despite the increase in backstreet abortions, which contribute to the high maternal mortality rate, particularly among adolescents. It is important that the government of Senegal adopts a less restrictive law regarding abortion.
Regarding adolescent births, early pregnancy is generally associated with high risks of death, both for mothers and newborns. The social consequences of adolescent pregnancies can also be serious, as they can compromise schooling and therefore personal development and independence. For these reasons, their birth rates are an important factor in the development of policies and the implementation of reproductive health strategies and programmes.
It was recently found that 14% of adolescent girls aged 10 to 17 in Senegal have already started their reproductive life [164] : 10% have had at least one child and 4% are pregnant with their first child. The proportion of adolescents who are or have been pregnant increases rapidly with age, from 1% at age 15 to 33% at age 19, at which age 26% of girls have already had at least one child. The proportion of girls who have already begun their reproductive life is much higher in rural areas (18%) than in urban areas (9%) and much lower in the West region than in the others (8% compared to a maximum of 20% in the South region). The earliness of pregnancy varies greatly with the level of education: 25% of young girls with no education have already begun their reproductive life, compared to 17% of girls at primary school level, and 7% of the most educated. Furthermore, young Senegalese girls experience inequality and discrimination, both because they are women and because they are young. This makes them particularly vulnerable to social realities, which leave little space for their needs to be expressed. Specific expectations weigh on these young girls’ sexuality, and tradition is concerned with the preservation of virginity, and therefore of non-procreation, until marriage.
The contraceptive prevalence rate in Senegal is 26%, compared to 10% in 2010–2011 [165] . The Siggil Jigéen Network has developed several programmes to mobilize domestic resources from local authorities to fund family planning. We obtained 107 million CFA francs in contributions from mayors as a commitment to directly fund FP. The Siggil Jigéen Network also recruited more than 1,000 reproductive age women [166] (RAW) to play a role in family planning (FP) in the communes involved and the signing of protocols with mutual health insurance companies to support post-partum family planning until 2019 in their locality. The Siggil Jigéen Network also advocated for an increase in the budget for the purchase of contraceptives, with a view to the budget being set at 300 million CFA francs compared to 200 million in 2016.
The association has also developed many other activities. As part of the Deliver for GOOD campaign, it set up a steering committee and an advisory committee that brought together seven ministries, in addition to the Secretary of State to the Minister of Justice: the Ministry of Health and Social Action, the Ministry of National Education, the Ministry of Petroleum and Energy, the Ministry of Women, Family, Gender and Child Protection, the Ministry of Culture and of Communication and the Ministry of Justice. Thus, the Minister of Family, Women, Gender and Child Protection committed to supporting the Deliver for Good Senegal campaign, a global advocacy campaign that aims to put women and girls at the centre of the implementation of Sustainable Development Goals (SDGs). The Siggil Jigéen Network also helped build the capacity of members and allies of the Deliver For Good coalition through its progamme, Enjeux des ressources énergétiques propres et fossiles : impacts et opportunités pour les femmes et les filles au Sénégal ("Clean and fossil energy resources: impacts and opportunities for women and girls in Senegal”), which helps mobilize resources from oil to finance gaps in health and education programmes. The association also produced a final report on the documentary review of access to information for young people on adolescent reproductive health (ARH) in secondary schools and colleges in the communes of Mbao, Keur Massar and Rufisque. The association also approved the pre-report of the documentary review for the update of the study conducted in 2017 on the review of the national family planning strategic framework (Additional FP plan for young people). To this end, it has recruited two certified expert consultants to conduct an oil and gas study. Finally, the association ensured that the presidential candidates included the Sustainable Development Goals SDG3 [167] , SDG4 [168] and SDG7 [169] in their programmes.
How do you think it would be possible to develop access to better sexual and reproductive health care for girls and women in your country? What are the obstacles encountered in developing such access?
Access to SRH services for girls and women requires a great deal of innovation and synergy from all stakeholders for effective multi-sectoral management of SRH. The aim is to set up a social and health dynamic that will enable people to reflect on their reasons for acting, establish dialogue and thus work on gender relations and provide support in a consistent manner for adolescents and young people. There is also a need to strengthen networking between actors working in the area of adolescent reproductive health and youth and thus create better synergies between the Ministry of Education, Youth, Women and Health, both at the policy and operational levels.
The Siggil Jigéen Network and other civil society organizations are working on this. However, there are barriers that make it difficult for girls and women to access SRH services. One of the first obstacles remains the health policy environment, notably the law on reproductive health (law no. 2005–18 of 5 August 2005) which has no implementing decree. There are no legal restrictions on young people’s access to contraception and other basic health services, such as pregnancy and sexually transmitted infection (STI) testing, except for the requirement that they must be at least 15 years old to consent to HIV testing. Senegal’s Penal Code states that induced abortion is not legal, even to save a woman’s life, and imposes heavy prison sentences and fines. However, many young women resort to backstreet abortions, which can often compromise their health. Issues relating to gender inequality and social norms, as well as lack of information, are major barriers to women’s access to SRH services.
What actions would you prioritize to ensure that more girls and women have access to health care facilities and information to enable them to know their rights, and thus fight against early marriages and pregnancy, female genital mutilation, gender-based violence, etc.?
Awareness-raising activities must be developed across the population thereby helping certain beliefs and preconceived ideas to be deconstructed. It is also necessary to continue to strengthen advocacy at government level to obtain the signature of the decree implementing the RH law and the enforcement of texts against forced marriages and female genital mutilation. The state needs to facilitate access to health insurance by reducing costs and including family planning services. There is also a need to continue advocacy for resource mobilization with local governments, as they can contribute to raising the country’s contraceptive prevalence rate by agreeing to fund SRH and family planning. In awareness-raising activities, it is necessary to join forces with religious traditional and cultural leaders, and also to involve men. In general, the priorities can be listed as follows:
Concerning young people, there is a need to:
– involve them in all stages of the development, implementation and monitoring of plans and strategies that affect them.
– include adolescents and young people who are not in school or have dropped out of school in SRHR outreach activities.
– mobilize young girls, including married girls (priority target).
Concerning communities and opinion leaders, there is a need to:
– continue and strengthen social mobilization experiments, in particular through innovative multi-channel campaigns.
– mobilize religious and traditional leaders in favour of family planning to drive changes in social norms.
– increase spaces for dialogue on population and development issues, with the inclusion of influential religious groups.
– strengthen mechanisms for identifying and referring cases of child marriage at community level.
At the political level, there is a need to:
– review legislative instruments that restrict the development of SRHR for adolescents and young people.
– to follow through on the commitments made to adolescents and young people in the FP Plan and at the Family Planning 2020 Summit in London.
– institutionalize the strengthening and scaling up of community-based approaches to SRHR/FP service delivery.
– support comprehensive sexuality education (CSE) programmes that are suited to and respectful of our values.
– soutenir la décentralisation des politiques et programmes de DSSR/PF au niveau des collectivités locales.
– support the decentralization of SRHR/FP policies and programmes at the local government level.
Concerning health structures, there is a need to:
– implement a comprehensive and integrated package of SRHR/FP/HIV services at all types of health facilities suited to adolescents and young people.
– make public and private health centres more adolescent and youth-friendly.
– train a critical mass of health workers in SRHR, gender and youth approaches, and provide support and training supervision for them.
– continue and strengthen experiments in community-based SRHR/FP provision to reach young people more effectively.
Concerning schools, there is a need to:
– continue to integrate comprehensive RH education modules that respect our values into the education system as specified in the strategic plan for sexual and reproductive health for adolescents and young people.
– improve teachers’ capacities to deal with SRHR issues.
Concerning communication, there is a need to:
– develop multi-channel social and political mobilization campaigns, with a particular focus on social media.
– use the C’est la vie! series as a tool for multi-channel communication campaigns (radio, radio and TV publicity, talk shows, awareness-raising caravans, debate screenings, etc.).
The commitment to gender equality is also reflected in information programmes for both men and women and awareness-raising projects on women’s rights involving men. What types of programmes should be funded?
Programmes managed by civil society organizations should focus on:
– expanding SRH services through innovative, context-specific and audience-specific strategies and improving quality through capacity building and community mobilization.
– improving the knowledge and abilities of adolescents and young people relating to SRHR with a view to reducing gender inequality, discrimination and violence and empowering them.
– Strengthening a favourable social and legal environment through awareness raising and advocacy with key actors (religious, traditional, and family) and the production of knowledge necessary for policy dialogue.
In other words, gender equality programmes that call for working in consortium should be reinforced. Health, entrepreneurship, education and agriculture are relevant areas. There is also a need to fund large-scale programmes aimed at social behavioural change to increase people’s understanding of the concepts of equality, gender and equity. Advocacy at the level of policy makers for the adoption of regulations favourable to women and girls’ development also needs to be further strengthened in terms of funding.
Schools also have a role to play in combating gender-based discrimination, sexual orientation, etc. and in promoting comprehensive sexuality education. What programmes are or could be developed in this direction in your country and, if they exist, are there any collaborations at the regional level?
We are involved in advocacy at the regional level and at the level of the ECOWAS (Economic Community of West African States) for the proposal of a legal act for gender equality to be effective in this area. In the current situation, the effective implementation of this legal instrument could greatly contribute to strengthening advocacy for the integration of this curriculum into school programmes. In West Africa, there has been evolution, notably in the participation of women in public life and in the political will shown by governments.
However, there are a lot of delays, harmonization difficulties and insufficient implementation of legal instruments. This situation is mainly due to the absence of specific texts for the sub-region, making it difficult to achieve synergy of action between governments and effective monitoring.
This led women’s networks, human rights organizations and their technical and financial partners to initiate a movement whose objective was the adoption by ECOWAS member states of a protocol to promote women’s rights in this area, similar to that of the SACD (Southern African Development Community). Thus, after a sustained advocacy process towards West African states for the adoption of a protocol proposed by women’s and human rights organizations from thirteen countries, including Burkina Faso, Guinea Conakry, Mali, Niger and Senegal, the ECOWAS member states adopted a very important legal instrument for the people.
The 47th Summit of the ECOWAS Heads of State and Government, held on 19 May 2015 in Accra, Ghana, adopted the additional act on equal rights between women and men, regarding which awareness has not been sufficiently raised.
What concrete commitments do you expect from the Generation Equality Forum, especially concerning the part devoted to the promotion of sexual and reproductive rights? What are the best funding channels in this area? Which international bodies do you find most effective in promoting SRHR?
Funding for SRH needs to be increased. This commitment could help countries because of the many challenges they face, including access to good-quality health care and services. Local organizations that have solid experience and can generate concrete results should be supported. The United Nations system, the AFD and Canadian cooperation are international bodies that appear to be effective in promoting SRHR.
2. People interviewed
The team working with Delphine O , ambassador and general secretary of the Generation Equality Forum: Benjamin Bechaz , Deputy Secretary General of the Generation Equality Forum, Julie Vignon , Editor for Sexual and Reproductive Health and Rights (SRHR), representative of the SRHR focal point for France, Ministry of Europe and Foreign Affairs, interviewed on 22 January 2021.
Mar Merita Blat , Gender Project Director, Lucie Broechler , Health Division, Anne Isambert , Gender Advisor, Demographic Transition Department at AFD, interviewed on 15 February 2021.
Générations Féministes Collective: Nicolas Rainaud , advocacy manager at Equipop, Sharlene Sezestre , international advocacy manager at Family Planning, Christine Mauget , international affairs manager at Family Planning, Marie Lussier , SRH programme manager at Médecins du Monde, interviewed on 10 March 2021.
Hubert Chauvet , CEO French Office Amref Health Africa, interviewed on 15 March 2021.
Laurianne Desquesses , advocacy manager, Yann Illiaquer , analysis and advocacy coordinator, for Global Health Action, interviewed on 23 March 2021.
Bruno Rivalan , Deputy Executive Director of Global Health Advocates, interviewed on 26 March 2021.
Maty Dia, Partnership Manager for the Global Financing Facility civil society hub, interviewed on 1 April 2021.
Fatou Ndiaye Turpin , Executive Director of the Siggil Jiggéen Network in Senegal, interviewed on 2 April 2021.
Wendyam Micheline Kaboré , Executive Director of the Initiative Pananetugri pour le Bien-être de la Femme au Burkina Faso (Pananetugri Women’s Well-Being Initiative in Burkina Faso), interviewed on 2 April 2021.
Ousmane Kadri Nouhou , Executive Director of the Niger Better Life Foundation, interviewed on 8 April 2021.
Clémence Schantz , midwife and doctor in sociology at the Institut de Recherche pour le Développement (IRD), interviewed on 9 April 2021.
Mélanie Vion , Head of Projects-Community Mobilization/Civil Society Partnerships for Solthis, interviewed on 13 April 2021.
Lesia Radelicki , member of the cabinet of Helena Dalli, European Commissioner for Equality, interviewed on 14 April 2021.
Oumou Salif Touré , member of the West African Young Feminists Network in Mali, interviewed on 15 April 2021.
Nafissa Hassan Alfari , President of the Nigerian Cell of Young Female Leaders, interviewed on 19 April 2021.
Anaïs Kintgen , project manager, civil society mobilization – Generation Equality Forum at the Ministry of Europe and Foreign Affairs and the Ministry of Gender Equality, interviewed on 22 April 2021.
Julie Vignon , Editor for Sexual and Reproductive Rights and Health, Population and Demography, Ministry of Europe and Foreign Affairs, interviewed on 22 April 2021.
Jean-Claude Mulunda , IPAS Director for the Democratic Republic of Congo (DRC), interviewed on 23 April 2021.
Sam Ntelamo , Head of Adis Ababa Office, Paulin Tra , Data, Strategy and Governance Officer in Nairobi, IPPF Africa, interviewed on 26 April 2021.
Pierre Crozier , Regional Advisor for Global Health at the French Embassy in Angola, Congo-Brazzaville, Gabon and the Democratic Republic of Congo (DRC), interviewed on 29 April 2021.
Jane Medor , Programme and Resource Mobilization Manager for JED (Senegal), member of the Alliance Droits et Santé Network, interviewed on 30 April 2021.
Norbert Coulibaly , Ouagadougou Partnership Senior Technical Manager, interviewed on 30 April 2021.
Abou Bakary Traoré , obstetrician-gynaecologist in Bamako, Mali, interviewed on 6 May 2021.
Irmine Ayihounton , member of the West African Young Feminists Network, interviewed on 07 May 2021.
Pierre-Alain Rubbo , Regional Global Health Advisor at the French Embassy in Burkina Faso responsible for Burkina Faso, Mali and Niger, interviewed on 10 May 2021.
Fleur Vernat , French Muskoka Fund Secretariat, interviewed on 11 May 2021.
Mar Merita Blat , Gender Project Director at the AFD, interviewed on 17 May 2021.
Laurence Rossignol , Senator, former Minister for Families, Children and Women’s Rights, interviewed on 20 May 2021.
Perri Sutton , Programme Officer in the Family Planning team at the Bill & Melinda Gates Foundation, interviewed on 3 June 2021.
Definition of SRHR: “Sexual and reproductive health and rights mean that people should have the right and the resources to make decisions about their reproductive and sexual lives free from coercion, discrimination and violence.” Source: International Planned Parenthood Federation, “Sexual and reproductive health and rights: the key to gender equality and women’s empowerment”, IPPF, 2015. ↑
“Les droits et la santé sexuels et reproductifs au cœur des politiques étrangères féministes” (Sexual and reproductive health and rights at the heart of feminist foreign policy), Joint position paper by Médecins du Monde, Equipop, Family Planning, May 2020. ↑
3 questions to Phumzile-Mlambo-Ngcuka, UN Women’s executive director, on gender equality around the world ahead of the Generation Equality Forum”, Focus 2030, 8 March 2021. ↑
« Covid-19: UN predicts disastrous impact of pandemic on women’s health », UN Info, 29 April 2020 ↑
“ L’Action extérieure de la france sur les enjeux de population, de droits et santé sexuels et reproductifs 2016–2020” (France’s external action on population, sexual and reproductive health and rights 2016–2020). Mid-Term Accountability Report, Directorate General for Global Affairs, Culture, Education and International Development, December 2018. ↑
Ibid . ↑
In view of the disparities between countries in sub-Saharan Africa on the issue of SRHR, we cannot claim to be exhaustive. We have therefore focused on countries in West African and Central Africa whose populations particularly suffer from the lack of resources devoted to SRHR and with which France has a special bilateral relationship. ↑
For the countries targeted by our study: Mali, Senegal, Burkina Faso, Niger and the Democratic Republic of Congo (DRC). ↑
Female genital mutilation covers all procedures including partial or total removal of the external female genitalia or any other injury to the female genitalia that is not performed for medical reasons. (Sources: WHO.) ↑
Recommendations for the ICPD beyond 2014: Sexual and Reproductive Health and Rights for All, High-level Task Force for the International Conference on Population and Development (ICPD), High- Level Task Force for ICPD, 2013. ↑
Interviews conducted with Oumou Salif Touré, a member of the West African Young Feminists Network for Mali, on 15 April 2021 and with Pierre Crozier, regional advisor on global health in Angola, Congo-Brazzaville, Gabon and DRC, on 29 April 2021. ↑
My body is my own. Claiming the right to autonomy and self-determination, United Nations Population Fund (UNFPA), 2021, pp.18–19. ↑
Ibid ↑
Ibid , p. 21. ↑
Akinrinola Bankole et al, From unsafe to safe abortion in sub-Saharan Africa: slow but steady progress, Guttmacher Institute, December 2020. ↑
Ibid ↑
The Democratic Republic of Congo is not one of the countries. ↑
Interview with Fatou Ndiaye Turpin, Executive Director of the Siggil Jigéen network in Senegal, on 2 April 2021. ↑
Interviews conducted with the Pananetugri Women’s Well-Being Initiative (IPBF) on 2 April 2021 and with Oumou Salif Touré, a member of the West African Young Feminists Network for Mali, on 15 April 2021. ↑
Olivier Dubois, “Au Mali, qui a peur du grand méchant genre” (“In Mali, who thinks gender equality is dangerous?”), Libération , 16 February 2021. ↑
Law n°2005–18 on reproductive health. ↑
Interview with Fatou Ndiaye Turpin, Executive Director of the Siggil Jigéen network in Senegal, on 2 April 2021. ↑
Interview with Oumou Salif Touré, member of the West African Young Feminists Network for Mali, 15 April 2021. ↑
My body is my own. Claiming the right to autonomy and self-determination , op. cit, p.136. ↑
Child Marriage: Latest trends and future prospects , UNICEF, July 2018, p. 4. ↑
"Thousands flee attacks by armed groups in eastern DRC”, UNHCR, 9 October 2020. ↑
Ginevra Vagliani, « Child marriage in sub-Saharan Africa: the case of Niger », Humanium, 1 December 2020. ↑
Interview with Nafissa Hassan Alfari, President of the Nigerian Cell of Young Female Leaders (CNJFL), 19 April 2021. ↑
Information provided by Ousmane Kadri Nouhou, Executive Director of the Niger Better Life Foundation on 8 April 2021. ↑
Interview with Oumou Salif Touré, member of the West African Young Feminists Network for Mali, 15 April 2021. ↑
Interview with Wendyam Micheline Kaboré, Executive Director of the IPBF, 2 April 2021. ↑
Interview with Maty Dia, Partnership Manager for the Global Financing Facility civil society hub, on 1 April 2021. ↑
Interview conducted with Pierre-Alain Rubbo, Regional Global Health Advisor at the French Embassy in Burkina Faso responsible for Burkina Faso, Mali and Niger, on 10 May 2021. ↑
Ibid ↑
« In some African countries, sizeable minorities of people live in polygamous households », Pew Research Center, 7 December 2020. ↑
Interview with Maty Dia, Partnership Manager for the Global Financing Facility civil society hub, on 1 April 2021. ↑
Fact sheets produced under the French Muskoka Fund, Equipop official site. ↑
Interview with the French Muskoka Fund, 11 May 2021. ↑
See PopulationData.net. ↑
Information provided by Fatou Ndiaye Turpin, Executive Director of the Siggil Jigéen Network in Senegal, March 2021. ↑
My body is my own. Claiming the right to autonomy and self-determination, op. cit. ↑
Interview with Clémence Schantz, midwife and doctor in sociology at the Institut de Recherche pour le Développement (IRD), 9 April 2021. ↑
Interview with Clémence Schantz, midwife and doctor in sociology at the IRD, on 9 April 2021. ↑
Interview with Irmine Ayihounton, member of the West African Young Feminists Network on ↑
Akinrinola Bankole et al., From unsafe to safe abortion in sub-Saharan Africa: slow but steady progress, op.cit. ↑
Ibid ↑
According to UNESCO statistics. ↑
Norbert Fiess and Arthur Gautier, Le financement du développement de l’Afrique subsaharienne à l’épreuve de la pandémie (Financing development in sub-Saharan Africa in the face of the pandemic), Trésor-Eco, no. 278, Direction Générale du Trésor, 9 March 2021. ↑
Protecting Women’s Health and Rights during Covid-19. Experiences and Feminist Perspectives from West African civil societyEquipop, 2020. ↑
Ibid . ↑
« Covid-19: UN predicts disastrous impact of pandemic on women’s health », UN Info, 29 April 2020 ↑
Ibid ↑
Comment un an de crise sanitaire et économique est venu accentuer les inégalités femmes-hommes (« How a year of health and economic crisis has accentuated gender inequalities »), Oxfam France, 5 June 2021. ↑
Interview with Maty Dia, Partnership Manager for the Global Financing Facility civil society hub, on 1 April 2021. ↑
Interview with Fatou Ndiaye Turpin, Executive Director of the Siggil Jigéen Network in Senegal, ↑
Interview with Jane Medor, Programme and Resource Mobilization Manager for Jeunesse et Développement (JED) in Senegal and member of the Alliance Droits et Santé network, on 30 April 2021. ↑
Interview with Nafissa Hassan Alfari, President of the CNJFL, 19 April 2021. ↑
Interview with Dr Jean-Claude Mulunda, IPAS Director for the DRC, 23 April 2021. ↑
Interview with Pierre Crozier, Regional Advisor on Global Health at the French Embassy in Angola, Congo-Brazzaville, Gabon and the Democratic Republic of Congo, 29 April 2021. ↑
Interview with Dr Jean-Claude Mulunda, IPAS Director for the DRC, 23 April 2021. ↑
Interview with Irmine Ayihounton, member of the West African Young Feminists Network on 7 May 2021. ↑
Interview with Dr Jean-Claude Mulunda, IPAS Director for the DRC, 23 April 2021. ↑
Interview with Maty Dia, Partnership Manager for the Global Financing Facility civil society hub, on 1 April 2021. ↑
Interview with Norbert Coulibaly, Ouagadougou Partnership Senior Technical Manager, 30 April 2021 ↑
Interview with Ousmane Kadri Nouhou, Executive Director of the Niger Better Life Foundation on 8 April 2021. ↑
Interviews with Nafissa Hassan Alfari, President of the CNJFL on 19 April 2021 and Oumou Salif Touré, member of the West African Young Feminists Network for Mali, on 15 April 2021 and with Ousmane Kadri Nouhou, Executive Director of the Niger Better Life Foundation on 8 April 2021. ↑
Interview with Oumou Salif Touré, member of the West African Young Feminists Network for Mali, 15 April 2021. ↑
Interview with Nafissa Hassan Alfari, President of the CNJFL, on 19 April 2021. ↑
Interview conducted with Oumou Salif Touré, member of the West African Young Feminists Network for Mali, on 15 April 2021 and with Nafissa Hassan Alfari, President of the CNJFL, on 19 April 2021. ↑
Interview with Oumou Salif Touré, member of the West African Young Feminists Network for Mali, 15 April 2021. ↑
Interview with Norbert Coulibaly, Ouagadougou Partnership Senior Technical Manager, 30 April 2021 ↑
Interview with Hubert Chauvet, CEO French Office Amref Health Africa, on 15 March 2021. ↑
Interview with Oumou Salif Touré, member of the West African Young Feminists Network for Mali, 15 April 2021. ↑
Now known as the Haut Conseil à l’égalité entre les femmes et les hommes (High Council for Equality between Women and Men). ↑
Stratégie genre et développement 2013–2017 focuses on sectoral indicators including sexual and reproductive health and rights. ↑
Stratégie genre et développement 2013–2017 (“Gender and Development Strategy 2013–2017”), Directorate-General for Global Affairs, Development and Partnerships of the Ministry of Europe and Foreign Affairs, p. 9. ↑
Évaluation formative sur l’engagement français Muskoka (Formative Evaluation of the French Muskoka Commitment) , Ministry of Europe and Foreign Affairs, 2020, p. 4. ↑
Directorate General for Globalization, Culture, Education and International Development, Mid-term Accountability Report, L’action extérieure de la France sur les enjeux de population, de droits sexuels et reproductifs 2016–2020 (France’s external action on population, sexual and reproductive rights issues 2016–2020), December 2018, p.14. ↑
See the map of the Ouagadougou Partnership projects: https ://map.partenariatouaga.org/ ?country=SN. ↑
Gender and the reduction of gender inequalities. Cross-cutting intervention framework 2014–2017, AFD, 2013, p. 20. ↑
« Press release by Laurence Rossignol at the 61st session of the Commission on the Status of Women at the UN in New York, 13 March 2017 », Ministry for Families, Children and Women’s Rights. ↑
Interview with Julie Vignon, Editor for Sexual and Reproductive Health and Rights, Population and Demography, Ministry of Europe and Foreign Affairs, 22 April 2021. ↑
Ibid . ↑
See the Discours d’Emmanuel Macron à l’occasion de la journée internationale pour l’élimination de la violence à l’égard des femmes et du lancement de la grande cause du quinquennat (Speech by Emmanuel Macron on the occasion of the International Day for the Elimination of Violence against Women and the launch of the major cause of the five-year term), Élysée, 25 November 2017. ↑
The Interministerial Committee on International Cooperation and Development (CICID) is a coordinating body, under the authority of the Prime Minister, which sets the guidelines for France’s development aid policy. See La politique d’aide au développement de la France (France’s development aid policy), Focus 2030, 21 April 2021. ↑
See Relevé de conclusions du Comité interministériel de la coopération internationale et du développement (CICID) (Statement of conclusions of the Interministerial Committee on International Cooperation and Development), Direction du Trésor, 8 February 2018. ↑
Ibid . ↑
Ibid . ↑
Stratégie internationale de la France pour l’égalité entre les femmes et les hommes (2018–2022) (France’s International Strategy for Equality between Women and Men) Ministry of Europe and Foreign Affairs, p. 31. ↑
Stratégie internationale de la France pour l’égalité entre les femmes et les hommes (2018–2022), op.cit., p. 32. ↑
Déclaration de vœux de Pascale Boistard, secrétaire d’État aux droits des femmes, sur l’égalité professionnelle, la parité et les droits des femmes (Statement by Pascale Boistard, Secretary of State for Women’s Rights, on work equality, parity and women’s rights) Paris 26 January 2016", Vie Publique. ↑
Draft law no. 574, adopted by the National Assembly on programming for solidarity development and the fight against global inequalities, National Assembly. ↑
Interview conducted with Pierre-Alain Rubbo, Regional Global Health Advisor at the French Embassy in Burkina Faso responsible for Burkina Faso, Mali and Niger, on 10 May 2021. ↑
Susan Faludi, Backlash. The Undeclared War against American Women , New York, Crown, 1991. ↑
Erika Guevara-Rosas, « Trump’s Global Gag: a Devastating Blow for Women’s Rights », Amnesty International, 25 January 2017. ↑
Delphine Sitbon, Décret anti-avortement: Trump signe, les députés européens s’indignent (Anti-abortion decree: Trump signs, MEPs indignant) , Le Courrier du Parlement, 20 March 2017. ↑
L’Action extérieure de la France sur les enjeux de population, de droits sexuels et reproductifs 2016–2020, op. cit. ↑
Les États-Unis refusent de laisser passer une résolution de l’ONU contre le viol comme arme de guerre (US refuses to pass UN resolution against rape as a weapon of war) Le Monde, 23 April 2019. ↑
Julien Lecot, Trente-deux pays se liguent contre le droit à l’avortemente (Thirty-two countries join forces against the right to abortion), Libération , 23 October 2020. ↑
L’Action extérieure de la France sur les enjeux de population, de droits sexuels et reproductifs 2016–2020 , op. cit. ↑
Stratégie internationale de la France pour l’égalité entre les femmes et les hommes (2018–2022), op. cit., p. 35. ↑
L’indispensable engagement de la France pour les droits et la santé sexuelle et reproductive. Positionnement Equipop, MDM et le Planning (France’s indispensable commitment to sexual and reproductive health and rights. Equipop , Médecins du Monde, and Family Planning Positioning), 17 January 2019. ↑
Francie Sadeski, Soheir Dani, Anne-Gaëlle Muths, Morgane Veillet Lavallée, Matthieu Lacave, Évaluation formative sur l’engagement français Muskoka (Formative Evaluation of French Muskoka Commitment) AFD, March 2020, p. 7. ↑
Évaluation formative sur l’engagement français Muskoka (2010–2017) (Formative Evaluation of the French Muskoka Commitment ), Technopolis, 30 October 2019. ↑
Donors Delivering Report , European Parliament Forum for Sexual and Reproductive Rights, 2020. ↑
Évaluation formative sur l’engagement français Muskoka (2010–2017), op. cit., p. 69. ↑
Ibid . ↑
Ibid , p. 7. ↑
The Creditor Reporting System is an OECD DAC database. ↑
Donors Delivering Report 2020, op. cit. ↑
L’Action extérieure de la France sur les enjeux de population, de droits sexuels et reproductifs 2016–2020, op. cit. ↑
Évaluation formative sur l’engagement français Muskoka, op. cit., p. 17. ↑
« Women and Young Girls », The Global Fund. ↑
L’Action extérieure de la france sur les enjeux de population, de droits et santé sexuels et reproductifs 2016–2020, op. cit. ↑
Interview with Laurianne Desquesses, Advocacy Manager, Yann Illiaquer, Analysis and Advocacy Coordinator, for Global Health Action, 23 March 2021. ↑
« French Aid Figures », Ministry of Europe and Foreign Affairs. ↑
Interview with Laurianne Desquesses Manager, Yann Illiaquer, Analysis and Advocacy Coordinator, for Global Health Action, 23 March 2021. ↑
Universal registration document , French Development Agency 2019, p. 30. ↑
Interview with the AFD, 17 May 2021. ↑
Minutes of the consultation meeting with civil society. Support Fund for Feminist Organizations (FSOP) , AFD, 31 March 2021. ↑
Ibid . ↑
Interview with the AFD, 17 May 2021. ↑
Interview with Equipop, Médecins du Monde and Family Planning, 10 March 2021. ↑
Interview with Bruno Rivalan, Deputy Executive Director of Global Health Advocates, 23 March 2021. ↑
European donor support to sexual & reproductive health & family planning. Trends analysis 2019–2020 , Countdown 2030 Europe, January 2021. ↑
Ibid . ↑
Protecting Women’s Health and Rights during Covid-19. Experiences and Feminist Perspectives from West African civil society, op. cit. ↑
Ibid . ↑
Ibid . ↑
Ibid . ↑
France’s International Strategy for Equality between Women and Men (2018–2022), op. cit. ↑
Interview with Maty Dia, Partnership Manager for the Global Financing Facility civil society hub, on 1 April 2021. ↑
John Bongaarts and Robert G. Potter, Fertility, Biology, and Behavior: An Analysis of the Proximate Determinants , New York, Academic Press, 1983. ↑
John Bongaarts, « Africa’s unique fertility transition », Population and Development Review , vol. 43, 2016, pp. 39–58. ↑
Assessments come from surveys conducted in the five countries and therefore provide a snapshot of the situation at the time of the survey, but not over a women’s entire fertility period. For sources, see notes on pages 105 and 108, corresponding to each of the five countries. ↑
Frank Lorimer and Meyer Fortes, Culture and Human Fertility: A Study of the Relation of Cultural Conditions to Fertility in Non-Industrial and Transitional Societies , Paris, UNESCO, 1954. Frank Lorimer was then Director of the Office of Population Research at Princeton University and Meyer Fortes, an Ashanti specialist, was a Professor of Social Anthropology at Cambridge. ↑
Senegal: Enquête de démographie et de santé continue 2018 (Ongoing Demographic and Health Survey) , Dakar, ANSD, 2019. ↑
Democratic Republic of Congo: Enquête de démographie et de santé 2013–2014 (Demographic and Health Survey), Kinshasa, Ministry of Planning, 2014. ↑
Mali: Enquête de démographie et de santé 2018 (Demographic and Health Survey), Bamako, INSTAT, 2019. ↑
Burkina Faso: Enquête de démographie et de santé et à indicateurs multiples 2010 (Multiple Indicator Demographic and Health Survey) , Ouagadougou, INSD, 2012. ↑
“Literacy”, UNESCO Institute for Statistics ↑
John Caldwell, Theories of Fertility Decline (Population and Social Structure), London, Academic Press, 1982. ↑
Child Marriage, Fertility, and Family Planning in Niger, Washington , Promundo, 2019. ↑
Niger: Multiple Indicator Demographic and Health Survey 2012 , Niamey, INS, 2013. ↑
Solène Lardoux and Étienne Van de Walle, “Polygyny and fertility in rural Senegal”, Population , vol. 58, n°6, 2003, pp. 717–743. ↑
Note, this was in 2013. ↑
Gary S. Becker, A Treatise on the Family, Cambridge (Mass.), Harvard University Press, 1981. ↑
Op. cit. , p. 50. ↑
Hervé Le Bras, “Après l’explosion démographique ”, Politique étrangère , No. 1, spring 2019, p. 107–121 (English translation: « After the Demographic Explosion », Cairn international). ↑
Hamidou Issaka Maga and Jean-Pierre Guengant, "Countries with very slow or incipient fertility transition” in Hans Groth and John F. May (eds) : Africa’s Population: In Search of a Demographic Dividend , New York, Springer, 2017, pp. 147–154. ↑
See Marita Kongo and Chardin Carel, Le protocole à la charte africaine des droits de l’homme et des peuples relatif aux droits des femmes en Afrique : état des lieux, (“Protocol to the African Charter on Human and Peoples’ Rights on the Rights of Women in Africa: the current situation”) Laval University, April 2019. ↑
Elizabeth A. Sully et al, Adding It Up: Investing in Sexual and Reproductive Health 2019 , Guttmacher Institute, 2020. ↑
The 2018 World Health Organization (WHO) report on the state of health in African regions. ↑
Executive summary: The impact of Covid-19 on women , United Nations, 9 April 2020. ↑
The abilities that enable us to cope with the demands and challenges of everyday life. ↑
Armand Kinda, "The Introduction of Homosexuality into Education: ‘It’s impossible!’ (Stanislas Ouaro)”, Minute.bf, 26 April 2021. ↑
This policy is widely known as the “global gag rule” because of the restrictions it places on the management of non-US government funds by the organizations concerned, including limiting the conversations health providers can have with their patients and preventing them from advocating for legal change in their own countries. ↑
According to the 2016 World Bank Report. ↑
See the Second Demographic and Health Survey (EDS-RDC II 2013–2014) , Ministry of Planning and Monitoring Implementation of the Revolution of Modernity and Ministry of Health, September 2014. ↑
See MICS DRC 2018 Report , Kinshasa School of Public Health Steering Committee. ↑
Sophie Chae, Patrick Kayembe, Jesse Philbin, Crispin Mabika and Akinrinola Bankole, The incidence of induced abortion in Kinshasa, Democratic Republic of Congo , Guttmacher Institute, October 2017. ↑
Clinical providers include clinicians (specialist or general practitioners, nurses, midwives), and anyone who is trained to provide clinical services in hospitals or health facilities. ↑
According to the National Health and Social Development Plan 2019–2028 , Ministry of Health and Social Action, Republic of Senegal. ↑
See Continuous Demographic and Health Survey (DHS-continuous), Key Indicators Report, 2019, Agence Nationale de la Statistique et de la Démographie (ANSD), Dakar, Senegal, November 2020. ↑
Ibid . ↑
AFP SMART Project, Réseau Siggil Jigean Report. ↑
“To ensure healthy lives and promote well-being for all people at all ages.” ↑
“To ensure inclusive and equitable quality education and promoting lifelong learning opportunities for all.” ↑
“To ensure access to affordable, reliable, sustainable and modern energy for all.” ↑